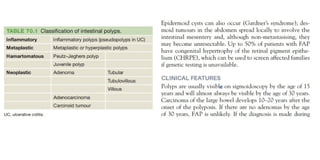
The document provides an overview of the small intestine, detailing its three parts: the duodenum, jejunum, and ileum, along with their structures, functions, blood supply, and innervation. It also discusses inflammatory bowel disease, specifically Crohn's disease, including its etiology, pathology, clinical features, and differences from ulcerative colitis. Medical tests and procedures related to small bowel health are also highlighted.













![• Clinical features
• ]A careful family history should be taken. Those with first-degree relatives who have developed colorectal cancer before the age of 45 years may be part of
one of the colorectal cancer familial syndromes.
• Tumours of the left side(distal ) of the colon usually present with a change in bowel habit or rectal bleeding,
• while proximal lesions typically present later, with iron deficiency anaemia or a mass (Figure 70.4). Patients commonly present with metastatic disease.
• Lesions of the flexures may present with vague upper abdominal symptoms for many months before symptoms suggestive of colonic disease appear.
• Investigation of colon cancer
• SCREENING
• In the UK, a screening programme has been introduced based on faecal occult blood testing of people aged 60–69 years, followed by colonoscopy in those
who test positive.
• A guaiac-based test is used, which detects peroxidase-like activity of faecal haematin. Studies have suggested a 15–20% reduction in colorectal cancer
specific mortality in the screened population. Flexible sigmoidoscopy can also be used as the initial screening tool, with a similar reduction in colorectal
cancer specific mortality.
• ENDOSCOPY
• The 60-cm, fibreoptic, flexible sigmoidoscope is increasingly being used in ‘one-stop’ rectal bleeding clinics.
• The patient is prepared with an enema and sedation is not usually necessary.
• It is usually possible to assess the bowel up to the splenic flexure, which will detect up to 70% of cancers and almost all that cause fresh rectal bleeding
(Figure 70.5).
• Colonoscopy is the investigation of choice if colorectal cancer is suspected, provided the patient is fit enough to undergo the mechanical bowel
preparation required. It has the advantage of not only picking up a primary cancer but also having the ability to detect synchronous polyps or other
carcinomas, which occur in 3–5% of cases.
• There is a small risk of perforation (1:1000).](https://image.slidesharecdn.com/smallandlargeintestine-241105190219-b158f90f/85/surgery-small-and-large-intestine-pptx-29-320.jpg)
![INFLAMMATORY BOWEL DISEASE
• The term ‘inflammatory bowel disease’ is reserved for conditions characterised by the presence of idiopathic intestinal inflammation (i.e. ulcerative colitis [UC] and Crohn’s disease [CD]. Although the availability of
population genetics andmolecular biology has contributed to our understanding of the pathogenesis of inflammatory bowel disease, the aetiology remains unclear. Ulcerative colitis UC is a disease of the rectum
and colon with extraintestinal manifestations. The incidence is 10 per 100000 per year in the UK with a prevalence of 160 per 100000 population. UC affects men and women equally in early life, although it is said
to be more common in males in later life. It is most commonly diagnosed between the ages of 20 and 40. UC is far more common in the USA and Western Europe but relatively rare in the Far East and tropics.
Asians who spent their childhood before the age of 14 in Asia have a much lower incidence of UC than Asians born and raised in the UK, suggesting an important effect of environmental exposure in childhood.
• Aetiology
• The cause of UC is unknown. There is clearly a genetic contribution, as 10–20% of patients have a first-degree relative with inflammatory bowel disease. Patients with severe colitis have a reduction in the number
of anaerobic bacteria and in the variability of bacterial strains in the colon, but no causative link with any specific organism has been identified. Unlike CD, smoking seems to have a protective effect in UC and has
even been the basis of therapeutic trials of nicotine. Relapses are occasionally said to be associated with periods of stress, but personality and psychiatric profiles in patients with UC are the same as those of the
normal population.
• Pathology
• In virtually all cases the disease starts in the rectum and extends proximally in continuity. Colonic inflammation is diffuse, confluent and superficial, primarily affecting the mucosa and superficial submucosa.
‘Pseudopolyposis’ occurs in almost one-quarter of cases. Stricturing in UC is very unusual (unlike CD) and should prompt urgent assessment because of the possibility of coexisting carcinoma. A small proportion of
patients develop irregular mucosal swellings (dysplasiaassociated lesions or mass [DALMs]), which are highly predictive of coexisting carcinoma. Histological examination reveals an increase in inflammatory cells
in the lamina propria and the crypts of Lieberkuhn and there are ‘crypt abscesses’. There is depletion of goblet cell mucin. With time, precancerous changes can develop (dysplasia). High-grade dysplasia is
regarded as an indication for surgery as 40% of colectomy specimens in which highgrade dysplasia was detected will have evidence of a colorectal cancer. In contrast, optimum management of low-grade dysplasia
is currently controversial. Ten to twenty per cent of patients with low-grade dysplasia will have a cancer at colectomy. The progression rate of low-grade dysplasia to invasive cancer is unclear and many cancers in
patients with low-grade dysplasia probably develop without high-grade dysplasia.
• Symptoms
• Clinical presentation depends in large part on the extent of disease. If confined to the rectum (proctitis), there is usually no systemic upset and extra-alimentary manifestations are rare. The main symptoms are
rectal bleeding, tenesmus and mucous discharge. The disease remains confined to the rectum in 90% of cases but proctitis may extend proximally. Colitis is almost always associated with bloody diarrhoea and
urgency. Severe and/or extensive colitis may result in anaemia, hypoproteinaemia and electrolyte disturbances. Pain is unusual. Children with poorly controlled colitis may have impaired growth. The more
extensive the disease the more likely extraintestinal manifestations are to occur. Extensive colitis is also associated with systemic illness, characterised by malaise, loss of appetite, and fever. Classification of colitis
severity The assessment of severity of UC is determined by frequency of bowel action and the presence of systemic signs of illness:
• ● Mild disease is characterized by fewer than four stools daily, with or without bleeding. There are no systemic signs of toxicity
• . ● Moderate disease corresponds to more than four stools daily, but with few signs of systemic illness. There may be mild anaemia. Abdominal pain may occur. Inflammatory markers, including erythrocyte
sedimentation rate and C-reactive protein, are often raised.
• ● Severe disease corresponds to more than six bloody stools a day and evidence of systemic illness, with fever, tachycardia, anaemia and raised inflammatory markers. Hypoalbuminaemia is common and an
ominous finding
• . ● Fulminant disease is associated with more than 10 bowel movements daily, fever, tachycardia, continuous bleeding, anaemia, hypoalbuminaemia, abdominal tenderness and distension, the need for blood
transfusion and, in the most severe cases, progressive colonic dilation (‘toxic megacolon’). This is a very significant finding, suggestive of disintegrative colitis, and an indication for emergency surgery if colonic
perforation is to be avoided.](https://image.slidesharecdn.com/smallandlargeintestine-241105190219-b158f90f/85/surgery-small-and-large-intestine-pptx-35-320.jpg)