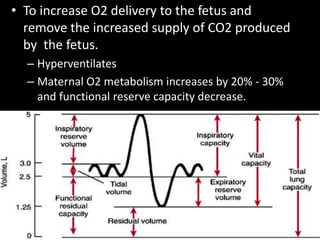
Downloaded 11 times
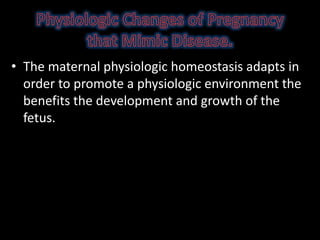
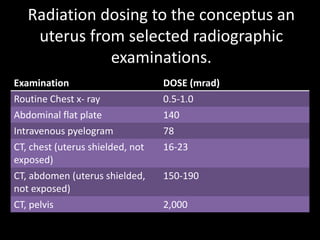
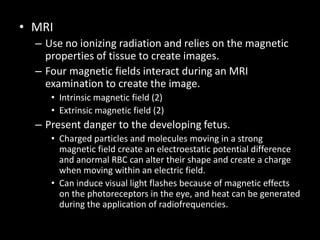
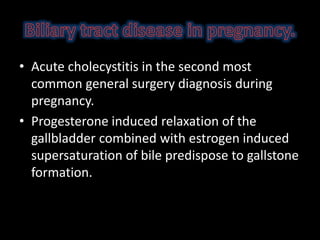
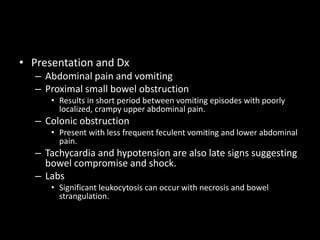
![Stimulates uterine
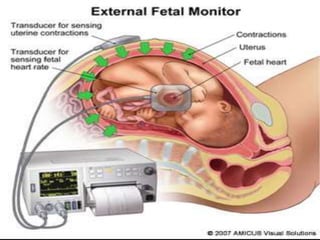
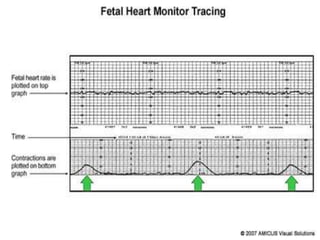
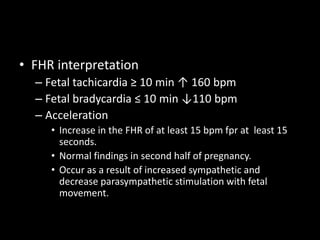
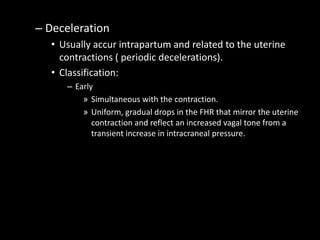
activity
Down regulates uterine
activity
Estrogen (opposing the action of
progesterone)
Progesterone (block Ca2+ flux
thought cell membrane)
Oxytocin ( secreted from posterior
pituitary. Stimulate Ca2+ across
myometrial plasma membrane and
distinct receptor myometrium and
other reproductive tissues.)
PGE₂, PGFα (favor activation of
the uterine musculature, onset uterine
contraction. Raise local [Ca2+] by
increasing release from intracellular
store. )
IL-1, IL-6 (produced locally by
placental tissue and act in concert with
other stimulatory factor)](https://image.slidesharecdn.com/thepregnantpatient-151205152340-lva1-app6892/85/The-pregnant-patient-11-320.jpg)
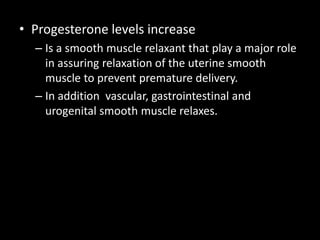
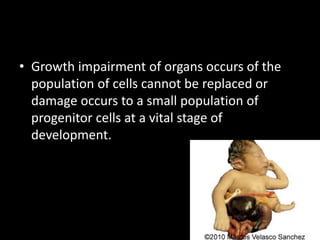
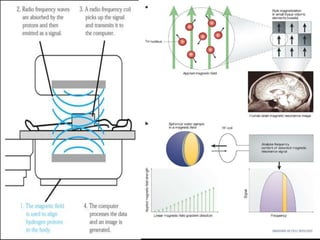
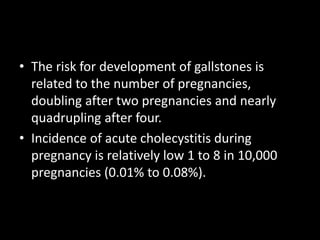
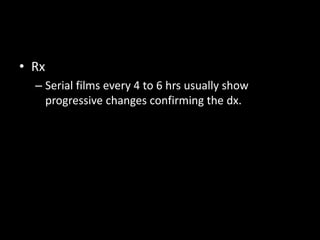
![• Magnesium sulfate
– First line tocolytic agent
– High intracellular [Mg] inhibits Ca2+ entry
myometrial cells interfering with actin-myosin
coupling. Also increase the sensitivity of K+
channels favoring hyperpolarization and uterine
relaxation.
– Range 4 and 9 mg/dL](https://image.slidesharecdn.com/thepregnantpatient-151205152340-lva1-app6892/85/The-pregnant-patient-14-320.jpg)
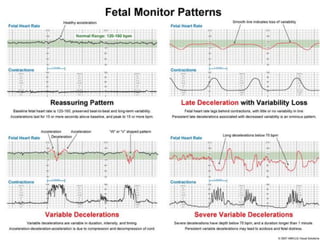
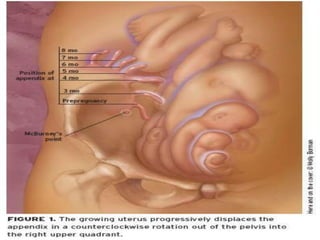
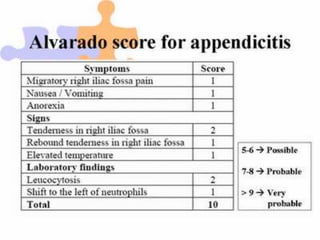




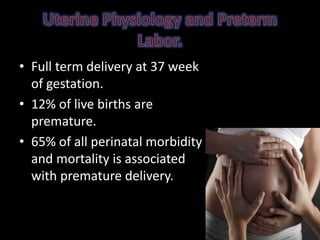
1. The document discusses physiological changes that occur during pregnancy including increased blood volume, cardiac output, and oxygen demand as well as changes in the gastrointestinal, cardiovascular and renal systems. 2. Fetal monitoring involves monitoring the fetal heart rate and uterine contractions to assess fetal well-being and response to stress. Fetal heart rate patterns including tachycardia, bradycardia, accelerations and decelerations are described. 3. Appendicitis is discussed as the most common nonobstetric surgical condition during pregnancy. Risks of appendicitis increase during pregnancy due to lymphoid hyperplasia in the appendix.


















![H:\Physiological Changes In Pregnancy[2]](https://cdn.slidesharecdn.com/ss_thumbnails/hphysiologicalchangesinpregnancy2-100305140624-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)





























![Obstetric physiology by dr shalini[208736]](https://cdn.slidesharecdn.com/ss_thumbnails/obstetricphysiologybydrshalini208736-170904022323-thumbnail.jpg?width=640&height=640&fit=bounds)






























