Downloaded 147 times


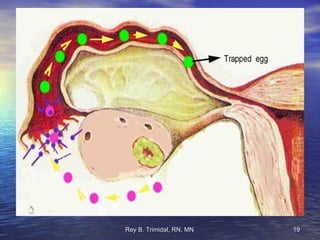
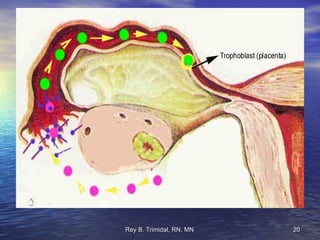
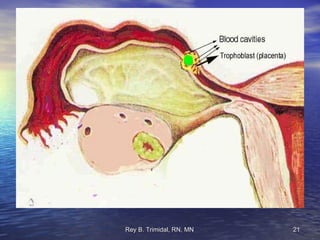
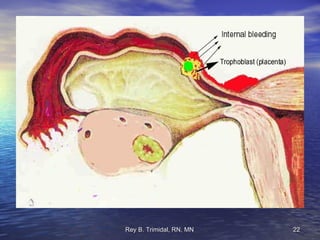


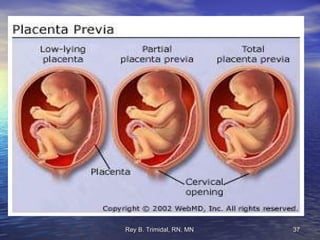

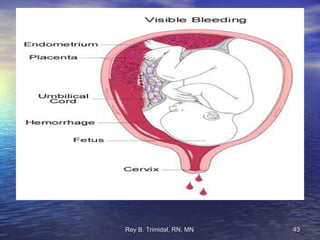
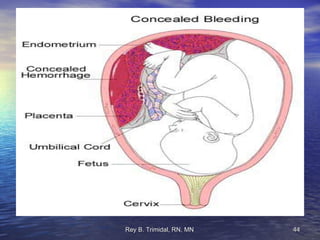




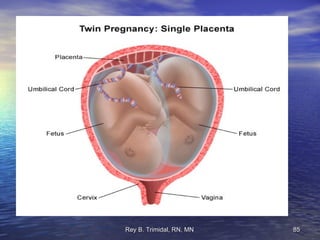
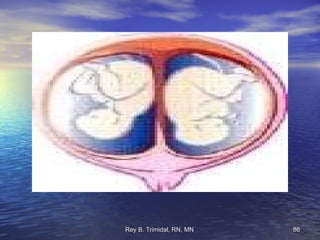







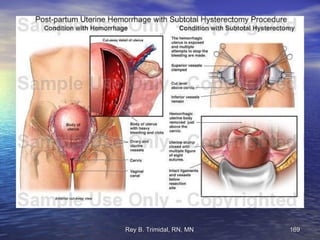








The document discusses various complications that can occur during pregnancy including hyperemesis gravidarum, bleeding during the 1st, 2nd and 3rd trimesters, ectopic pregnancy, molar pregnancy, premature rupture of membranes, dystocia, preterm labor, multiple pregnancy, pregnancy induced hypertension, cardiovascular disease, diabetes mellitus, and medical diseases complicating high risk pregnancy. It provides assessments, nursing interventions, and management for each complication.



















































![maternal guide presentation [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/maternalpresentationautosaved-250208125838-a01bbc1b-thumbnail.jpg?width=640&height=640&fit=bounds)


































