03/04/2025 2
OUTLINE
• INTRODUCTION
•CARDIOVASCULAR SYSTEM CHANGES
• RESPIRATORY SYSTEM CHANGES
• HAEMATOLOGICAL CHANGES
• GASTROINTESTINAL SYSTEM CHANGES
• RENAL SYSTEM CHANGES
• CENTRAL NERVOUS SYSTEM CHANGES
• ENDOCRINE SYSTEM CHANGES
• FACTORS AFFECTING PLACENTAL TRANSFER OF DRUGS
• ANAESTHETIC DRUGS
• CONCLUSION
• REFERENCES
3.
03/04/2025 3
INTRODUCTION
• Pregnancyis associated with significant adaptive changes in most of
the organ systems of the maternal body.
• The basis of most changes are hormonal, being in response to the
marked changes in the hormones associated with pregnancy.
• Most of the changes are in place in the first trimester but may
increase in intensity as pregnancy progresses.
4.
03/04/2025 4
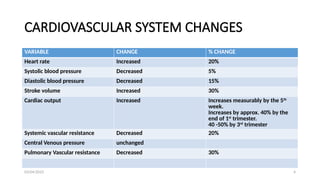
CARDIOVASCULAR SYSTEMCHANGES
VARIABLE CHANGE % CHANGE
Heart rate Increased 20%
Systolic blood pressure Decreased 5%
Diastolic blood pressure Decreased 15%
Stroke volume Increased 30%
Cardiac output Increased Increases measurably by the 5th
week.
Increases by approx. 40% by the
end of 1st
trimester.
40 -50% by 3rd
trimester
Systemic vascular resistance Decreased 20%
Central Venous pressure unchanged
Pulmonary Vascular resistance Decreased 30%
5.
03/04/2025 5
ANAESTHETIC IMPLICATIONS
CVSEXAM
• ANATOMY- The heart is displaced upward and to the left by the gravid uterus.
• Physical examination of the term pregnant woman may also be abnormal with the
auscultation commonly revealing a wide, loud 1st heart sound , an S3 sound and soft
systolic ejection murmur.
• So it is necessary to differentiate abnormal cardiac changes from Normal physiological
changes of pregnancy
• Criteria to diagnose cardiac disease during pregnancy:
1) Presence of diastolic murmur
2) Systolic murmur of severe intensity (grade 3)
3) Presence of severe arrhythmias , atrial fibrillation or flutter
6.
03/04/2025 6
CVS EXAM2
• Systemic vascular resistance(SVR) is decreased due to vasodilatory
effect of progesterone and proliferation of low vascular resistance
vascular beds in the intervillous spaces of placenta.
• BP is decreased due to decrease in SVR.
• ECG shows Left axis deviation, ST segment depression and T wave
flattening due to cephalad movement of diaphragm.
• Blood flow- to uterus increases up to 700mls/min by term.
• - increases to kidney and skin
• - remains same to brain and liver
7.
03/04/2025 7
ANAESTHETIC IMPLICATIONSCONTD
AORTOCAVAL Compression
• Enlarged uterus compresses IVC and Lower Aorta when the patient lies supine.
Obstruction of IVC decreases venous return which then leads to decrease in
cardiac output.
• It can occur as early as the 13th
week of pregnancy.
• When awake most women are capable of compensating for the decrease in
stroke volume by increasing Sytemic Vascular Resistance and Heart rate. There
are also alternative venous pathways : the paravertebral and azygos systems.
• During Anaesthesia compensatory mechanisms are reduced or abolished.
• Obstruction of lower aorta causes reduced blood flow to kidneys,
uteroplacental unit and lower extremities.
8.
03/04/2025 8
SUPINE HYPOTENSIONSYNDROME
• It is seen in 8 to 15% of pregnant women, they have Overt Caval
Compression (supine hypotension syndrome) characterized by;
Hypotension, Sweating, Bradycardia, Pallor, Nausea and Vomiting
• Prevention of SHS: Uterus should be displaced by placing a rigid
wedge under the right hip or left lateral tilting of the operating
table.
9.
03/04/2025 9
RESPIRATORY SYSTEMCHANGES
• Changes in the respiratory system during pregnancy involves the
upper airway, minute ventilation, lung volume , oxygen consumption.
• Major changes occurs in the respiratory system during pregnancy, due
to combination of both hormonal and mechanical factors.
• The maternal respiratory pattern changes as the uterus enlarges :-
Diaphragm rises up by 4 cm , causes reduction in the Functional
residual capacity by 20% patient prefers thoracic breathing over the
Abdominal.
• Due to increased metabolic demands, Oxygen consumption and
minute volume increases (40- 50%) progressively.
03/04/2025 11
ANAESTHETIC IMPLICATIONS
•Decreased FRC and Increased oxygen consumption promotes rapid
oxygen desaturation during periods of apnea. This is more marked in
obese patients and during anaesthesia.
• Preoxygenation prior to induction of general anesthesia is therefore
mandatory to avoid hypoxemia in pregnant patients.
12.
03/04/2025 12
Factors increasingrisk of hypoxaemia
• There is venous/capillary engorgement and edema of the upper airway
down to the pharynx, false cords, glottis and arytenoids.
• The increase in chest diameter and enlarged breasts can make
laryngoscopy difficult.
• There is reduced diaphragmatic movement.
• Failure to intubate the trachea is 7 times more common in the term
parturient compared to non pregnant patients.
• A smaller diameter endotracheal tube may be required for intubation
especially in cases of pre eclampsia.
13.
03/04/2025 13
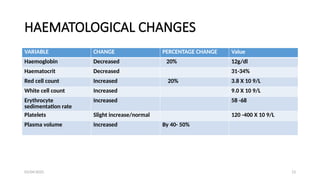
HAEMATOLOGICAL CHANGES
VARIABLECHANGE PERCENTAGE CHANGE Value
Haemoglobin Decreased 20% 12g/dl
Haematocrit Decreased 31-34%
Red cell count Increased 20% 3.8 X 10 9/L
White cell count Increased 9.0 X 10 9/L
Erythrocyte
sedimentation rate
Increased 58 -68
Platelets Slight increase/normal 120 -400 X 10 9/L
Plasma volume Increased By 40- 50%
14.
03/04/2025 14
COAGULATION CHANGES
•A state of hypercoagulability exists during pregnancy
• This is probably, a protective adaptation to lessen the risk of acute
haemorrhage that occurs at delivery.
• There is an increase in the majority of clotting factors, decrease in
quantity of natural anticoagulants and a reduction in fibrinolytic
activity.
• The platelet count remain remains unchanged throughout most of
pregnancy, but it may get reduced in third trimester.
• Despite the changes Bleeding time, prothrombin time and partial
thromboplastin time remain within normal limits.
15.
03/04/2025 15
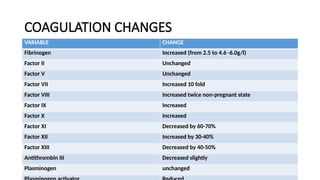
COAGULATION CHANGES
VARIABLECHANGE
Fibrinogen Increased (from 2.5 to 4.6 -6.0g/l)
Factor II Unchanged
Factor V Unchanged
Factor VII Increased 10 fold
Factor VIII Increased twice non-pregnant state
Factor IX Increased
Factor X Increased
Factor XI Decreased by 60-70%
Factor XII Increased by 30-40%
Factor XIII Decreased by 40-50%
Antithrombin III Decreased slightly
Plasminogen unchanged
16.
03/04/2025 16
ANAESTHETIC IMPLICATIONS
•There is increased risk of epidural haematoma in preeclampsia due
exponential fall in platelets. Thus, platelet count should done within
6 hours before placing epidural and removal of the catheter
• Standard heparin(unfractionated) preparation prophylaxis in low
doses i.e. 5000 I.U. Subcutaneously can be used in pregnancy, as it
does not cross the placenta.
• For performing the neuraxial block 4-6 hr gap after the last
dose,should be given.
17.
03/04/2025 17
ANAESTHETIC IMPLICATION(cont’d)
• In case of epidural anesthesia, catheter removal should be done 1 hr
prior to the next dose or 3-4 hr after the dose.
• Neuraxial anesthesia should be avoided in patient on the I.V.
heparin with increased Partial thromboplastin time.
• If the patient is started on heparin after placement of catheter,
removal of catheter is to be done after evaluation of the coagulation
profile.
18.
03/04/2025 18
• Lowmolecular weight heparin -Neuraxial block should be
performed after the minimum gap of 12 hr from the last dose (if
receiving higher dose e.g. enoxaparin 1mg/kg neuraxial block should
be performed after 24 hr gap).
• Platelet count should be obtained in the patient receiving LMWH to
prevent heparin induced thrombocytopenia.
• Post-op LMWH can be started only after 12 hr from the spinal
needle insertion.
• Use of oral anticoagulants is restricted as these agents can cross
placenta.
19.
03/04/2025 19
GASTROINTESTINAL(GI) SYSTEMCHANGES
• The changes in the GI stems from the effect of progesterone and
mechanical changes.
• Upward & anterior displacement of the stomach by the uterus leads
to increase in intragastric pressure and decrease in gastroesophageal
angle.
• Reduction of lower esophageal sphincter pressure due to the effect
of progesterone.
• Risk of Regurgitation and aspiration of gastric contents due to lower
oesophageal sphincter pressure. This may occur in at least 80% of
pregnant women.
20.
03/04/2025 20
• Theonset of GI symptom is from 16-20th
week of gestation and by
24th
hr post delivery progesterone falls to non pregnant level while
reflux usually resolves by 36th
hr.
• Increased placental gastrin secretion which can worsen gastric
acidity.
• GI motility is decreased but gastric emptying is believed to not be
delayed.Due to increase in transit time in small and large intestine,
there might be constipation.
21.
03/04/2025 21
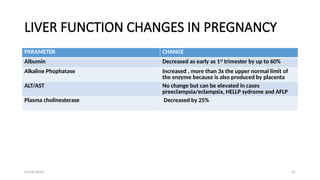
LIVER FUNCTIONCHANGES IN PREGNANCY
PARAMETER CHANGE
Albumin Decreased as early as 1st
trimester by up to 60%
Alkaline Phophatase Increased , more than 3x the upper normal limit of
the enzyme because is also produced by placenta
ALT/AST No change but can be elevated in cases
preeclampsia/eclampsia, HELLP sydrome and AFLP
Plasma cholinesterase Decreased by 25%
22.
03/04/2025 22
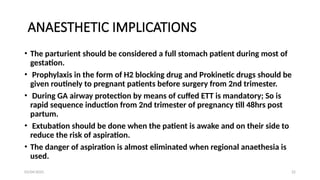
ANAESTHETIC IMPLICATIONS
•The parturient should be considered a full stomach patient during most of
gestation.
• Prophylaxis in the form of H2 blocking drug and Prokinetic drugs should be
given routinely to pregnant patients before surgery from 2nd trimester.
• During GA airway protection by means of cuffed ETT is mandatory; So is
rapid sequence induction from 2nd trimester of pregnancy till 48hrs post
partum.
• Extubation should be done when the patient is awake and on their side to
reduce the risk of aspiration.
• The danger of aspiration is almost eliminated when regional anaethesia is
used.
23.
03/04/2025 23
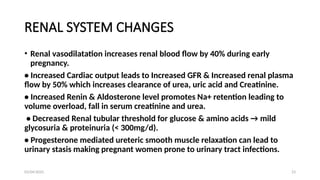
RENAL SYSTEMCHANGES
• Renal vasodilatation increases renal blood flow by 40% during early
pregnancy.
• Increased Cardiac output leads to Increased GFR & Increased renal plasma
flow by 50% which increases clearance of urea, uric acid and Creatinine.
• Increased Renin & Aldosterone level promotes Na+ retention leading to
volume overload, fall in serum creatinine and urea.
• Decreased Renal tubular threshold for glucose & amino acids → mild
glycosuria & proteinuria (< 300mg/d).
• Progesterone mediated ureteric smooth muscle relaxation can lead to
urinary stasis making pregnant women prone to urinary tract infections.
24.
03/04/2025 24
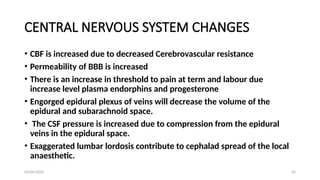
CENTRAL NERVOUSSYSTEM CHANGES
• CBF is increased due to decreased Cerebrovascular resistance
• Permeability of BBB is increased
• There is an increase in threshold to pain at term and labour due
increase level plasma endorphins and progesterone
• Engorged epidural plexus of veins will decrease the volume of the
epidural and subarachnoid space.
• The CSF pressure is increased due to compression from the epidural
veins in the epidural space.
• Exaggerated lumbar lordosis contribute to cephalad spread of the local
anaesthetic.
25.
25
• 25-40% decreasein minimum alveolar concentrations (MAC)
secondary to increased levels of progesterone and β- endorphin
levels which will lead to rapid induction with inhalation agents.
• The amount of local anaesthetic drug required in a pregnant woman
is decreased by up to 30% (2/3) compared to the non pregnant
state.
• Increased sensitivity to opiods, sedatives, and local anaesthetics
when used for neuraxial anaesthesia.
03/04/2025
26.
03/04/2025 26
ENDOCRINE SYSTEM
•Preganancy is Diabetogenic as insulin steadily rises during pregnancy and the human
placental lactogen (aka human chorionic Somatomamotropin) causes relative insulin
resistance.
• Pregnancy is biochemically a starving like state (blood glucose and amino acids are low
and Free fatty acids , ketones and triglycerides are high) to promote the Foetal growth.
• Secretion of HCG and Elevated oestrogen levels promotes hypertrophy of the thyroid
gland.
• There is increased in the production of thyroid globulin: although T3, T4 levels are
elevated up to 50% but the free T3, T4 & TSH remain normal due to increase production
THYROID BINDING GLOBULIN
• Level of PARATHYROID HORMONES and serum Ca++
tend to fall during pregnancy but the
level of ionized Ca++
tend to remain constant due changes in serum albumin concentration
27.
03/04/2025 27
• Thereis 30% increase in oxytocin store in the pituitary which is
released during labour
• There is hyperprolactinaemia due to placenta lactogen and
dopamine during pregnancy
• GA can mask the signs and symptom of hypoglycaemia while
neuraxial anaesthesia can worsen the haemodynamic instability due
to autonomic dysfunction related to DM
28.
03/04/2025 28
MUSCULOSKELETAL SYSTEM
•Exaggerated lumbar lordosis with flexion of the neck and downward
movement of the shoulders
• Due to relaxin, progesterone and mechanical effects of pregnancy, joint
laxity is increased to prepare for child birth
Implication
• Lordosis can decrease the distance between the spinous processes and
make neuraxial techniques difficult
• Widening of pelvis causes head down position in lateral decubitus and
lead cephalad position of LA during SAB in lateral position
• A pillow placed under the dependent position can counteract this effect
29.
03/04/2025 29
FACTORS AFFECTINGPLACENTAL TRANSFER
OF DRUGS
• Lipid Solubility:- The placental membrane is freely permeable to
lipid soluble substances, higher the solubility higher is the drug
transfer. Highly ionized substances have poor lipid solubility.
• Protein binding:- Protein bound drugs will not diffuse easily, only
free drug would cross the placental barrier easily , reduced albumin
levels will increases the unbound portion of drug in plasma.
• Maternal drug concentration :- Directly proportional , Affected by
the dose and route of administration.
• Others factors include: tissue binding, pH, pKa and blood flow
30.
03/04/2025 30
ANAESTHETIC DRUGS
•OPIODS– All opioids cross the placenta in significant amounts. They are weak
bases, bound to α-glycoprotein.
• Pethidine – Longer half life is due to its active metabolite norpethidine, which
may lead to respiratory depression in the neonate.
• Morphine – It is water soluble but readily crosses the placenta due to low
protein binding.
• Fentanyl – It is highly lipid soluble and albumin bound, so crosses the
placental barrier easily.
• IV Induction agents – Sodium thiopentone is highly lipid soluble, weakly
acidic, 75% protein bound and less than 50% ionized at physiological pH. It
crosses the placenta easily. Propofol – It is highly protein bound and lipophilic.
31.
03/04/2025 31
• INHALATIONALAGENTS-These agents are highly soluble with low
molecular weights.
• All cross placenta
• Muscle relaxants – These are quaternary ammonium compounds and
fully ionized with low lipid solubility, hence they do not cross the
placenta.
• Local Anaesthetics – These drugs have low molecular weights and also
are lipid soluble. The materno-foetal transfer is enhanced by foetal
acidosis leading to ion trapping.
• Different drugs have different protein binding.
32.
03/04/2025 32
CONCLUSION
• Pregnancyproduces profound physiological changes that alter the
usual responses to Anesthesia .
• Unique challenges - two patients are cared for simultaneously .
• Failure to take care can be disastrous for one or both of them.
33.
03/04/2025 33
REFERENCES
• JohnF,David M,John W: Morgan and Mikhail’s Clinical
anaesthesiology 5th
edition
• Alan R.A,Ian K.M,Jonathan P.T: Smith&Aitkenhead’s textbook of
anaesthesia 6th
edition,2014
• Peter K,Ian P: Principles of phyiology for the Amaesthetist,4th
edition
• Lee CY: Manual of Anaesthesia, MGH Education, 2006
• Steve MY, Nicholas PH, James KI: Anaesthesia, Intensive Care And
Perioperative Medicine (A-Z), 6th
edition






![Obstetric physiology by dr shalini[208736]](https://cdn.slidesharecdn.com/ss_thumbnails/obstetricphysiologybydrshalini208736-170904022323-thumbnail.jpg?width=640&height=640&fit=bounds)






















![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


















