
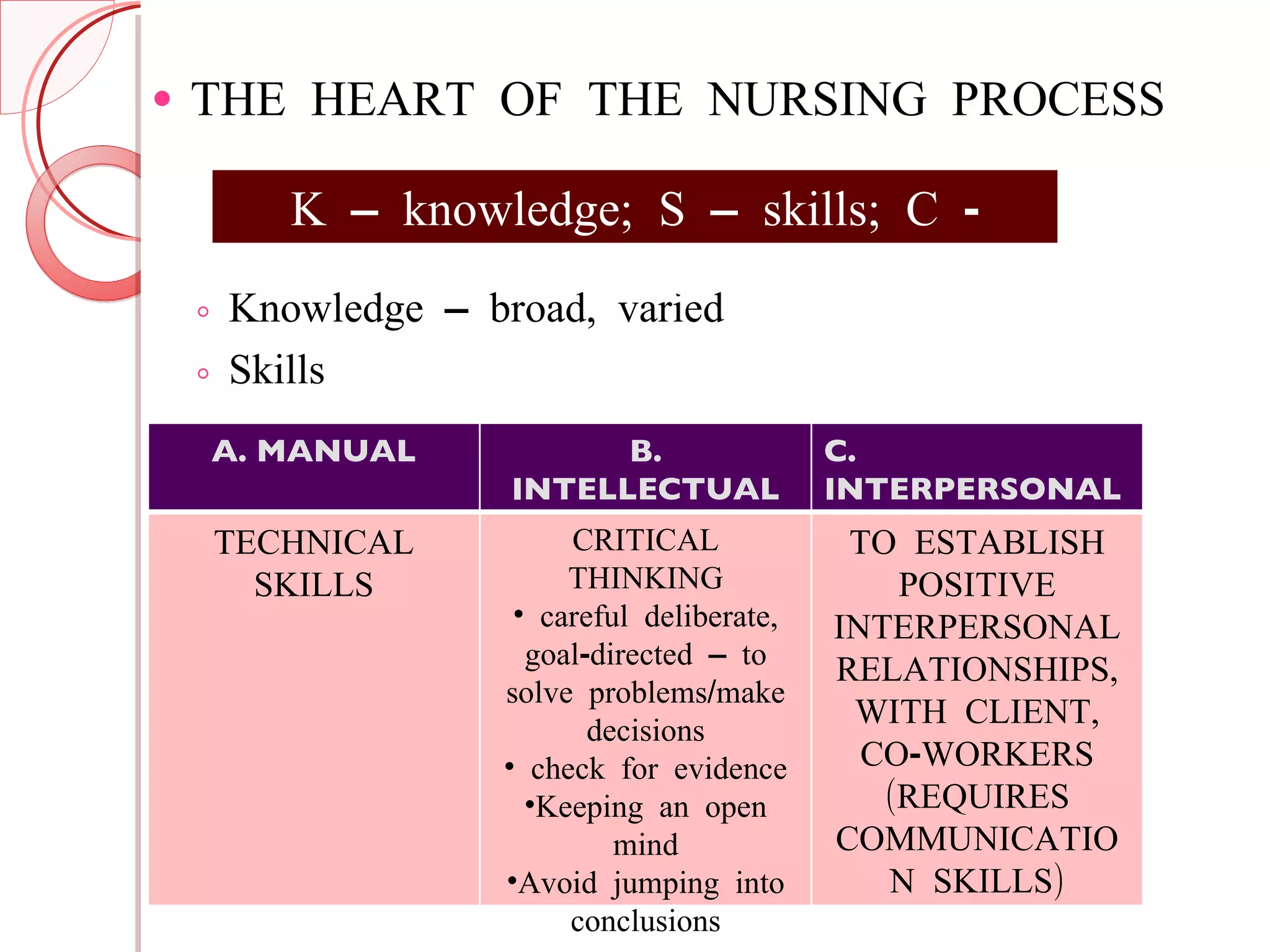
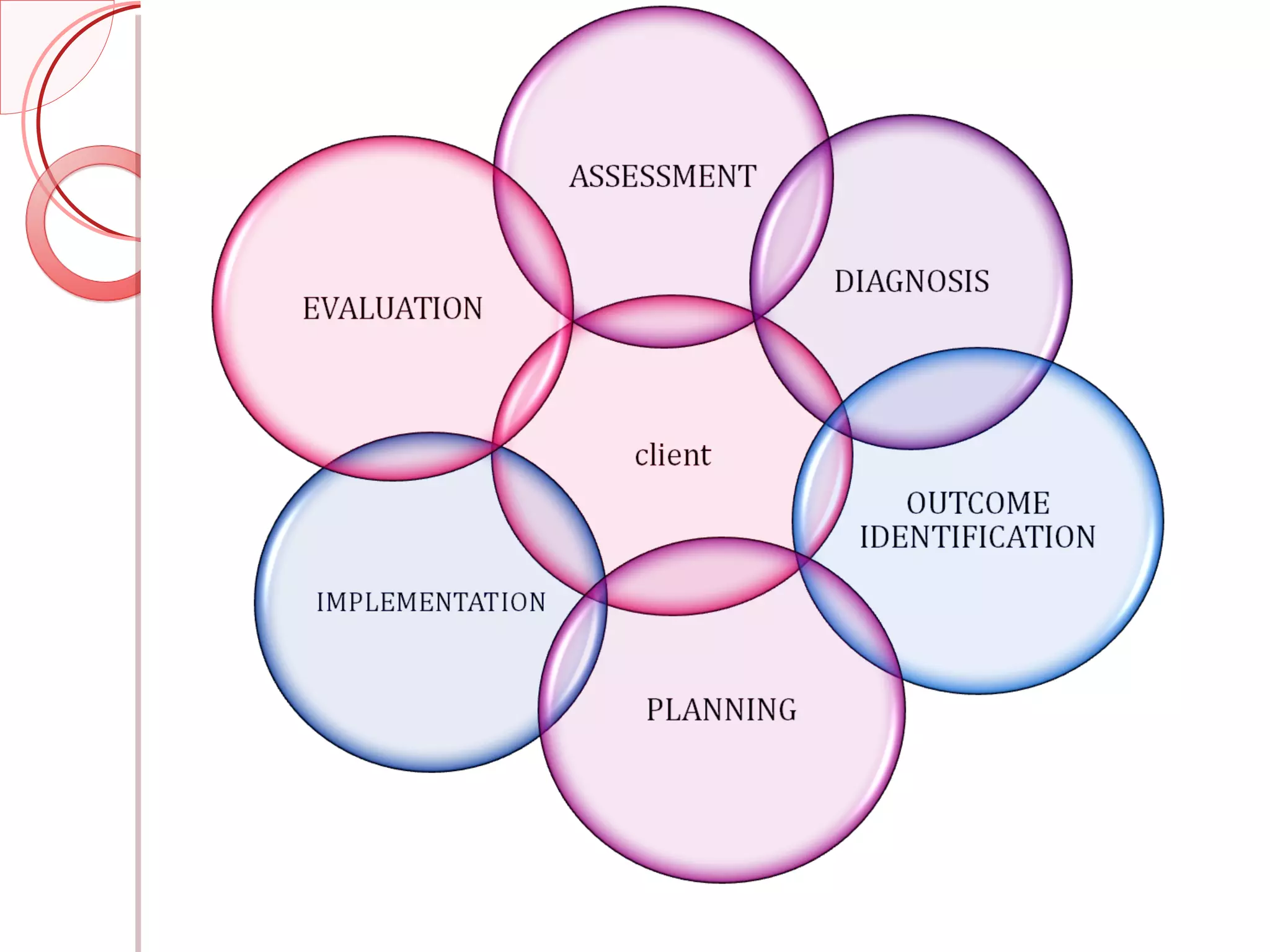

The nursing process includes assessment, diagnosis, planning, implementation, and evaluation. It is a systematic and organized way to provide individualized patient care. The nursing process involves collecting subjective and objective data, formulating nursing diagnoses, identifying goals and outcomes, planning interventions, implementing the care plan, and evaluating the effectiveness of the interventions. It benefits both patients and nurses by ensuring quality care and promoting professional development.






















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)