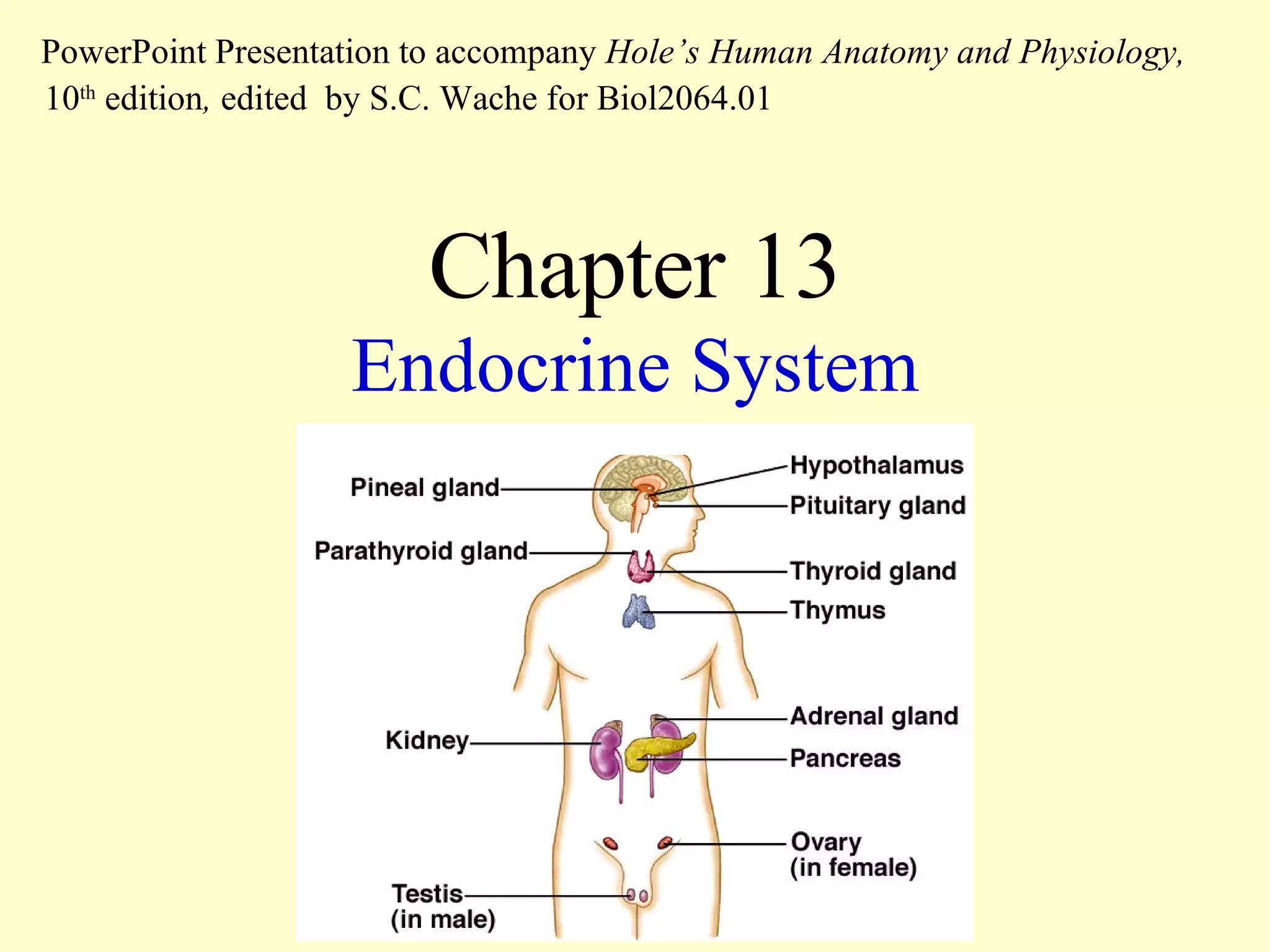
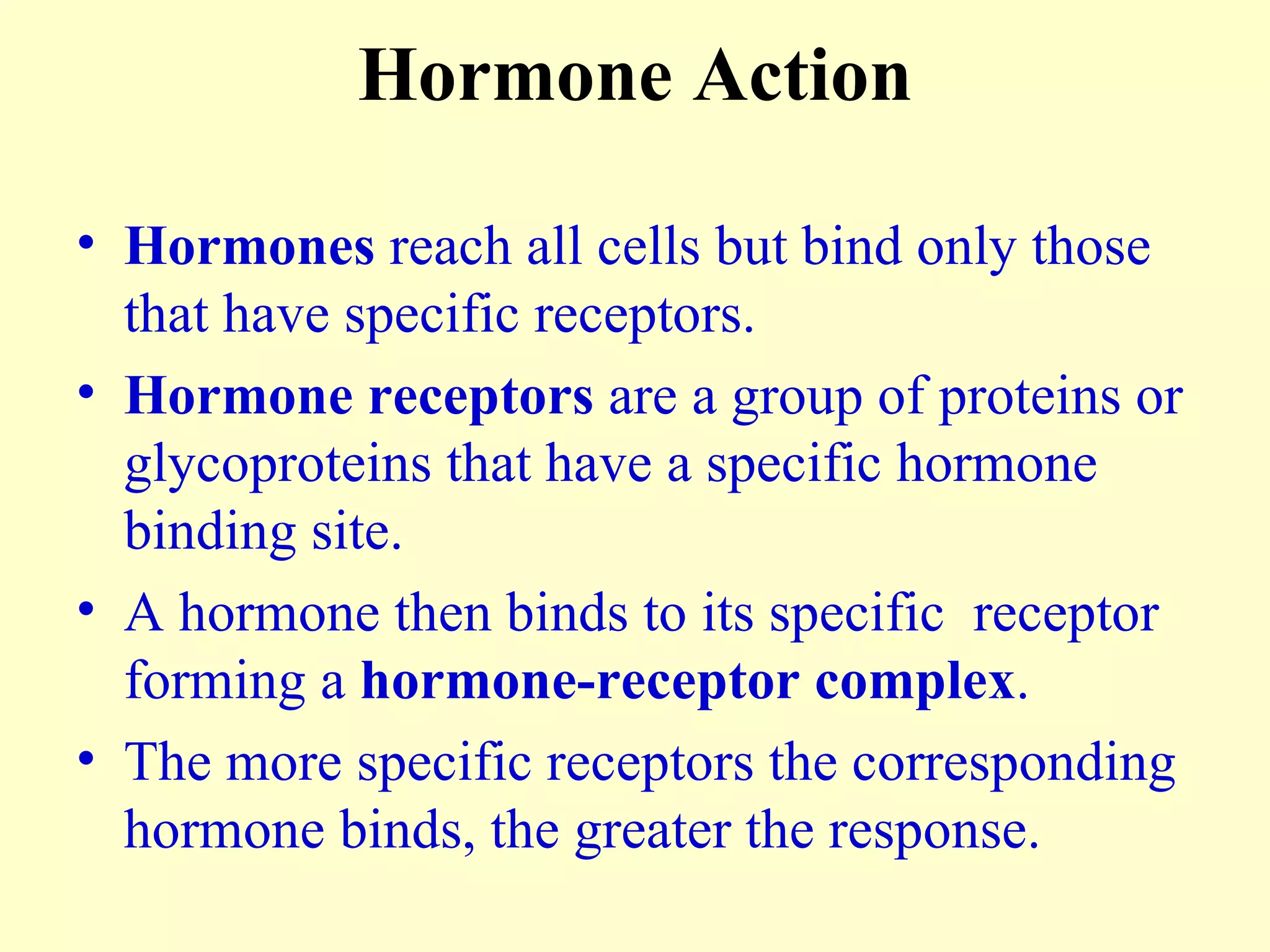
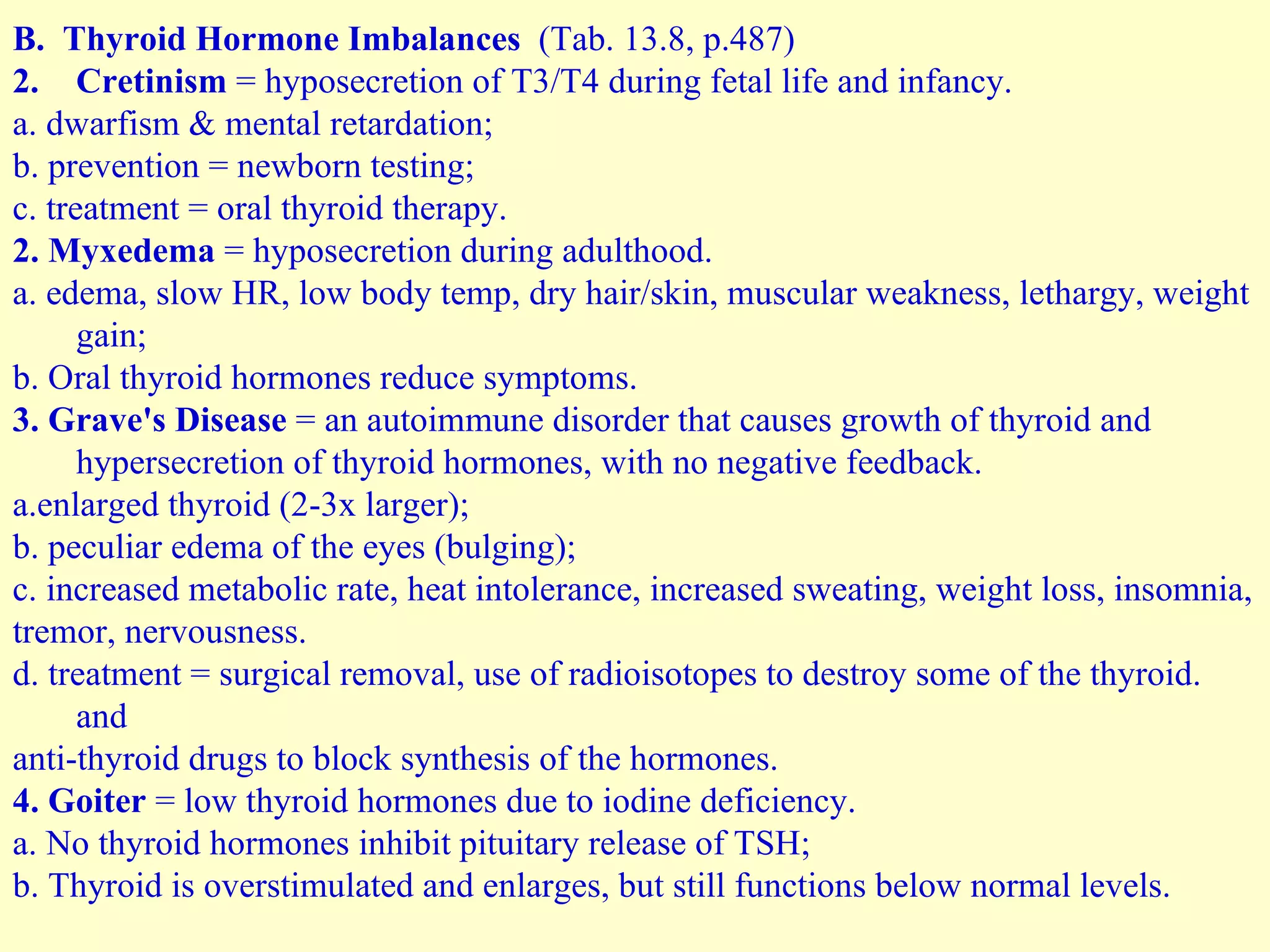
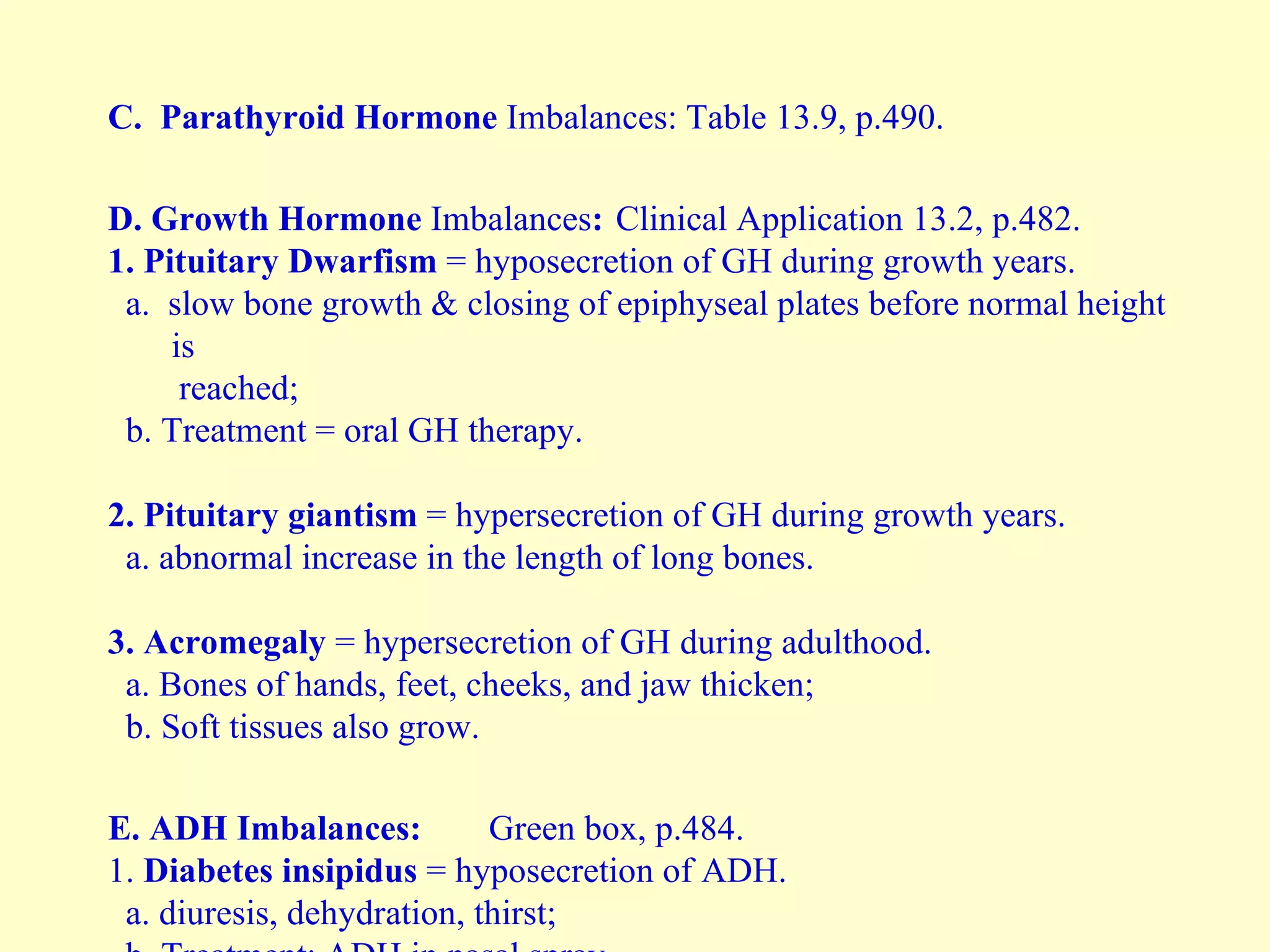
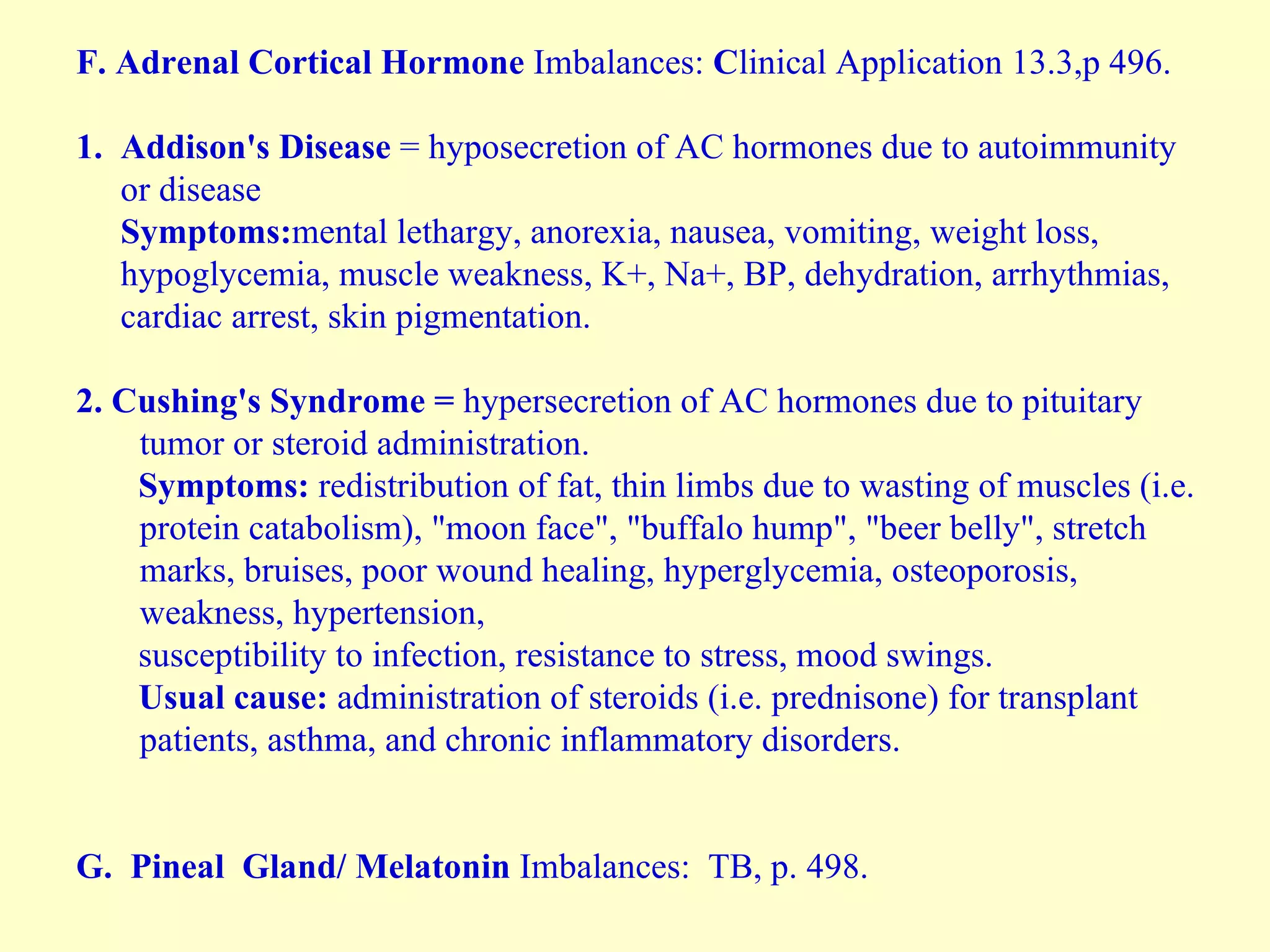
The document discusses the endocrine system and various endocrine glands. It provides information on the location and function of the hypothalamus and pituitary gland in controlling other endocrine glands. Key glands covered include the thyroid gland, parathyroid gland, adrenal gland, and pancreas. For each gland, the document describes their location in the body, the hormones they secrete, and the functions of those hormones in maintaining homeostasis.
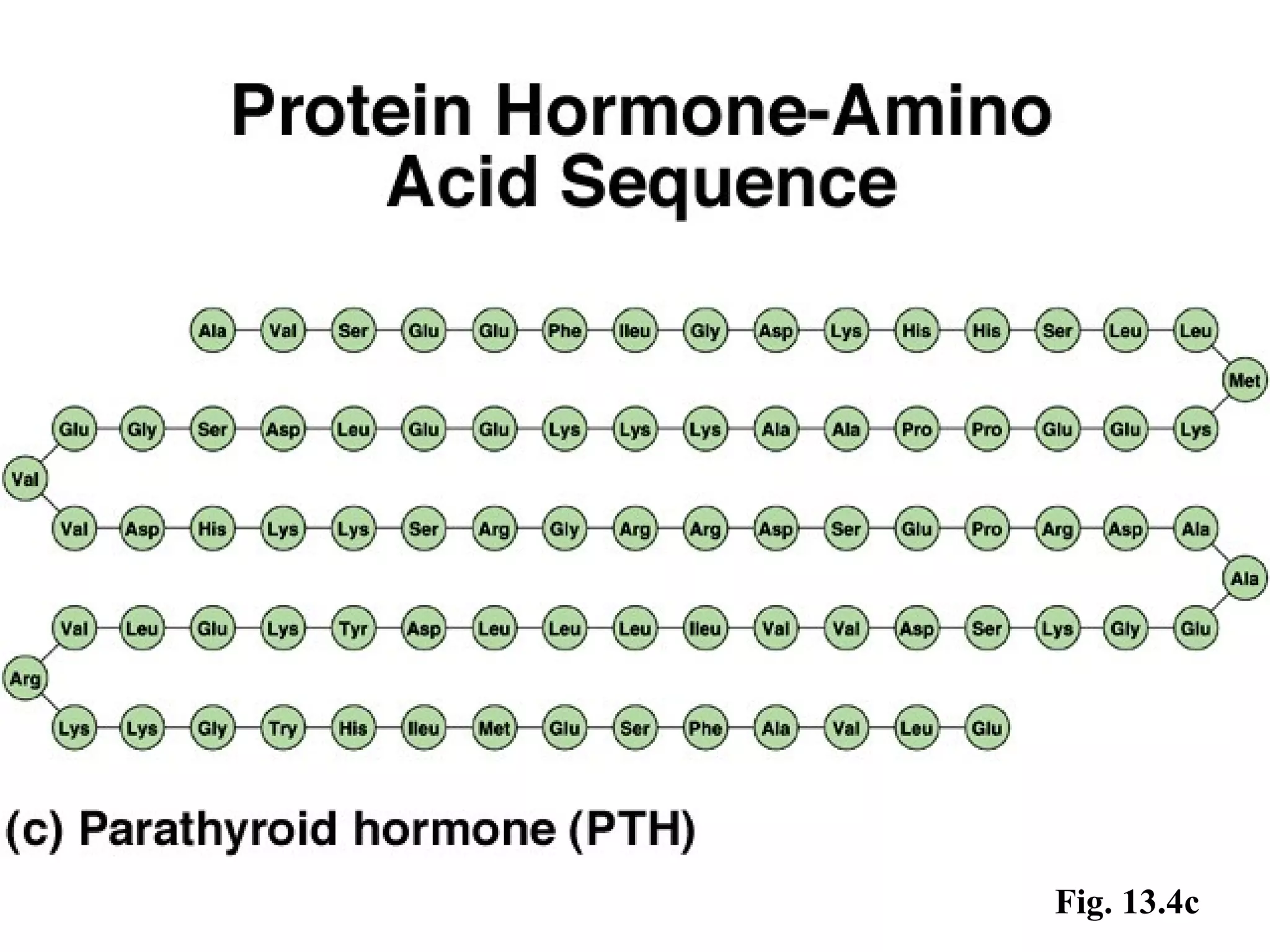
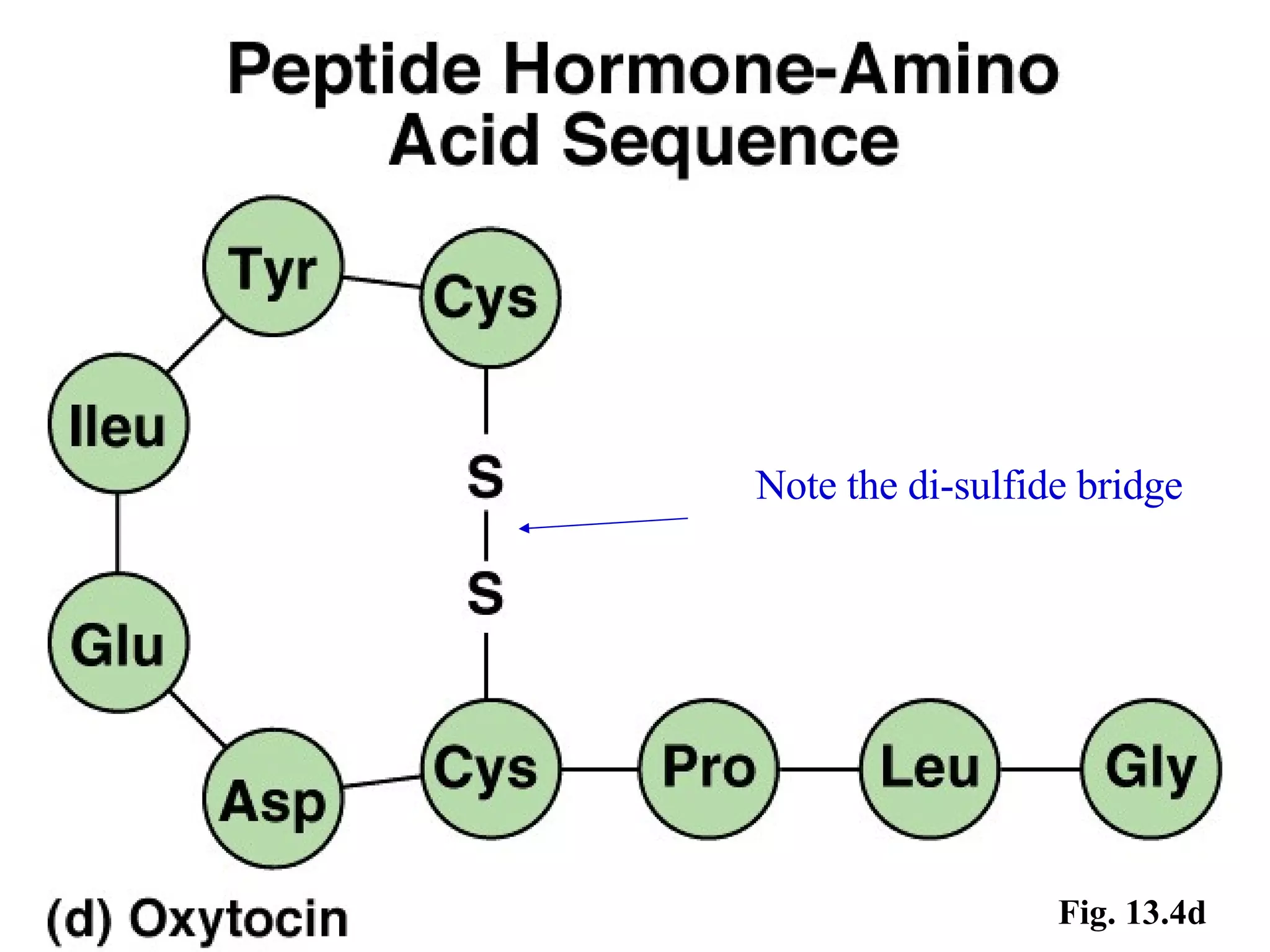
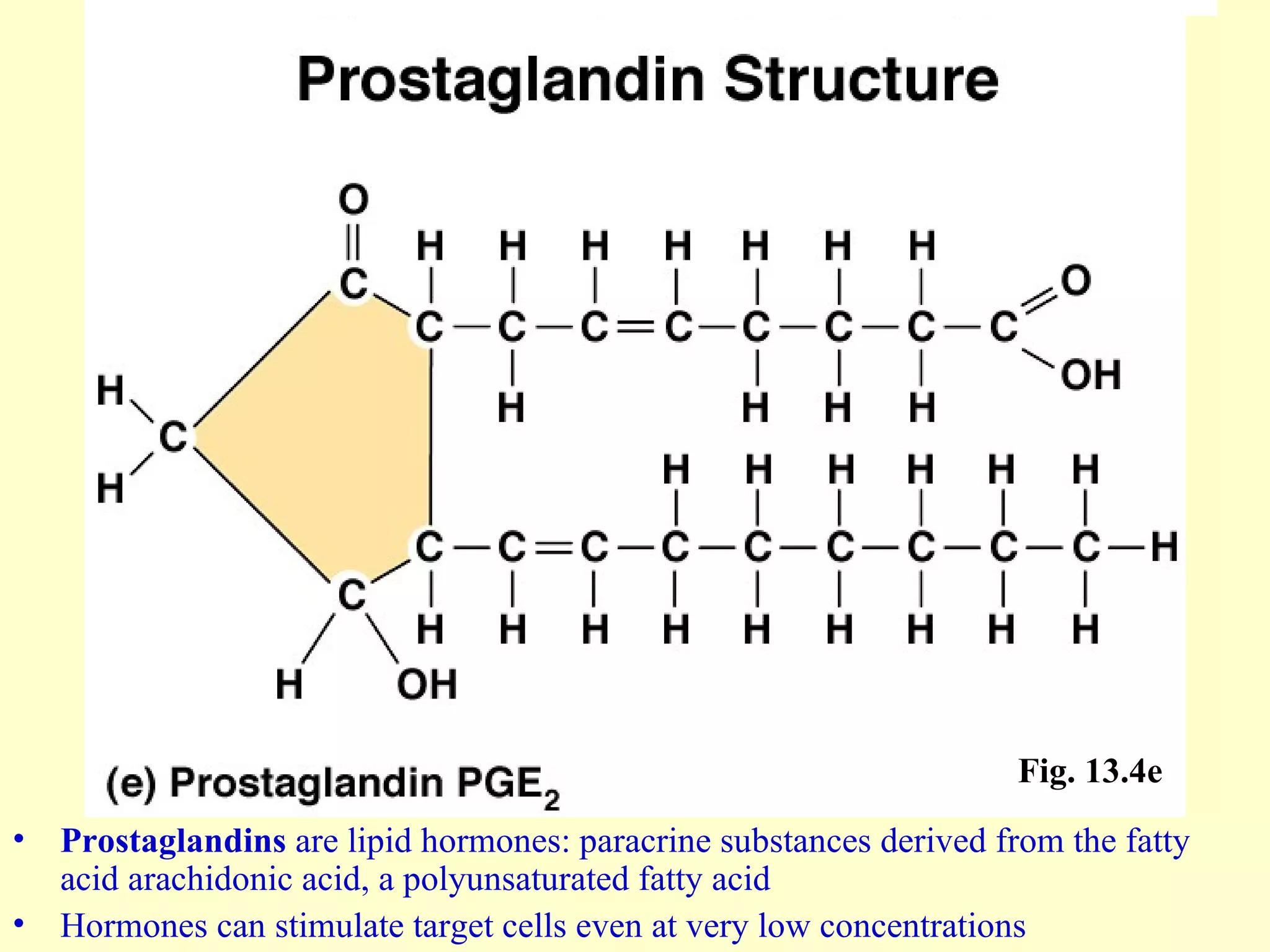
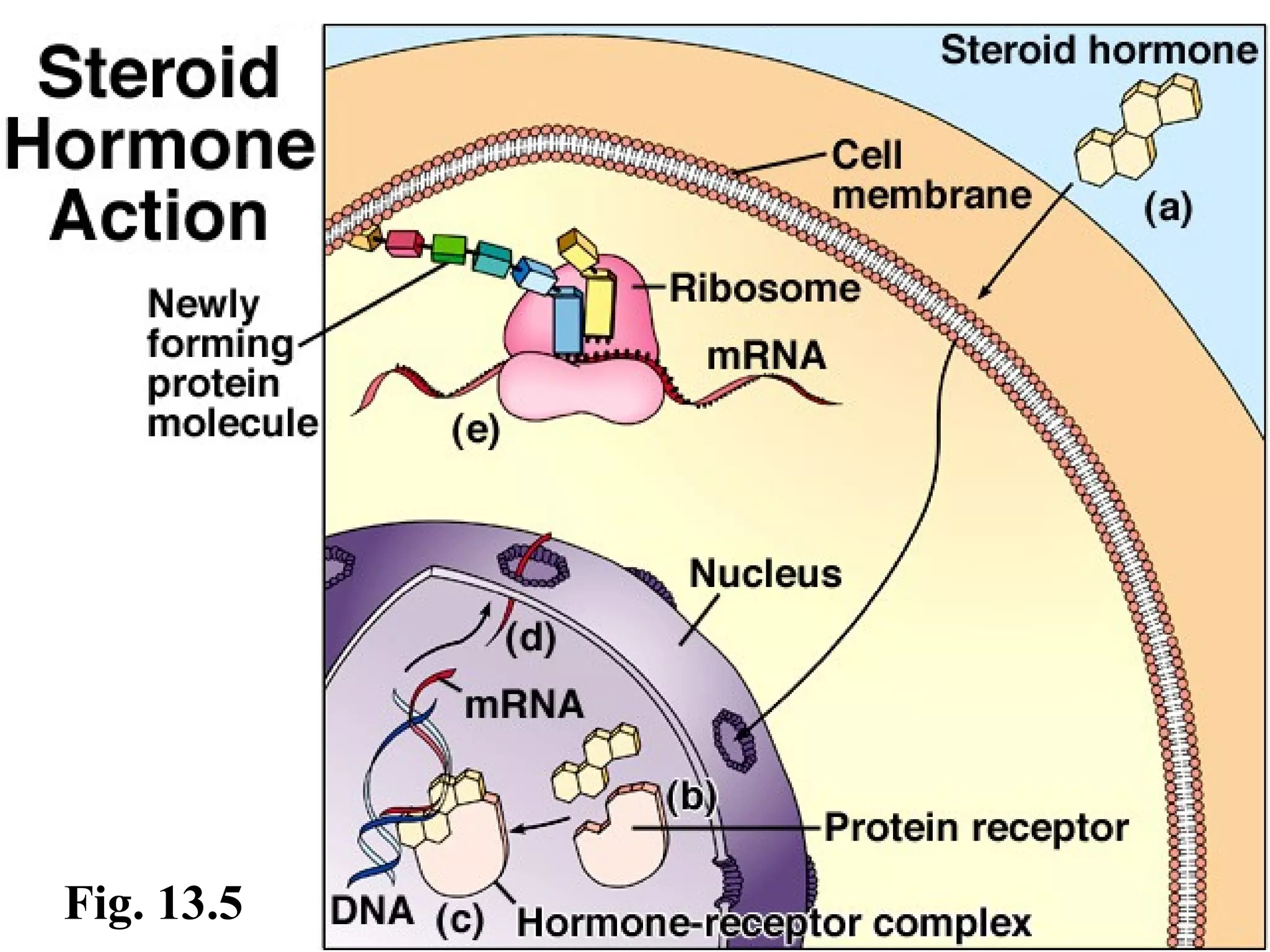
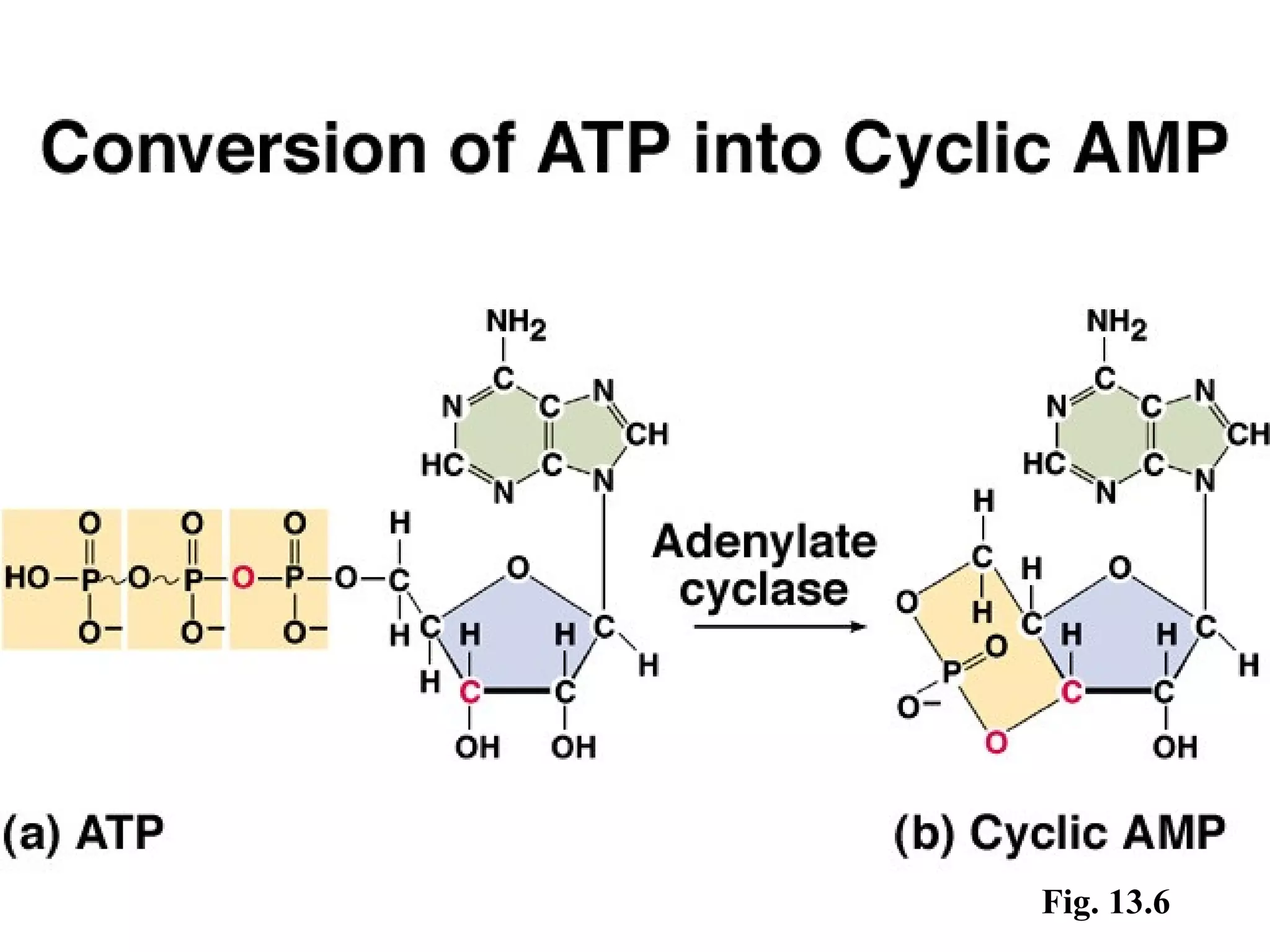
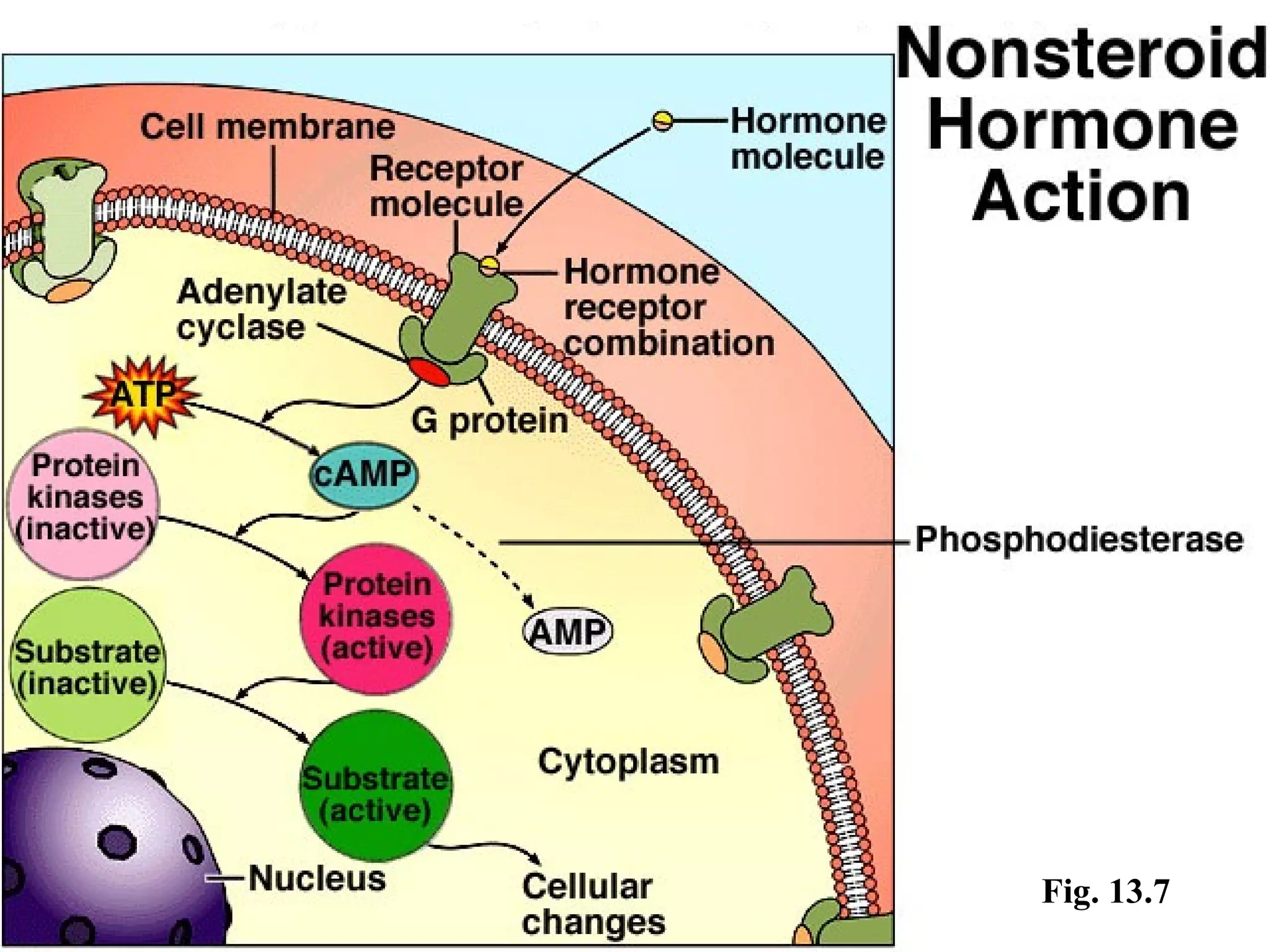
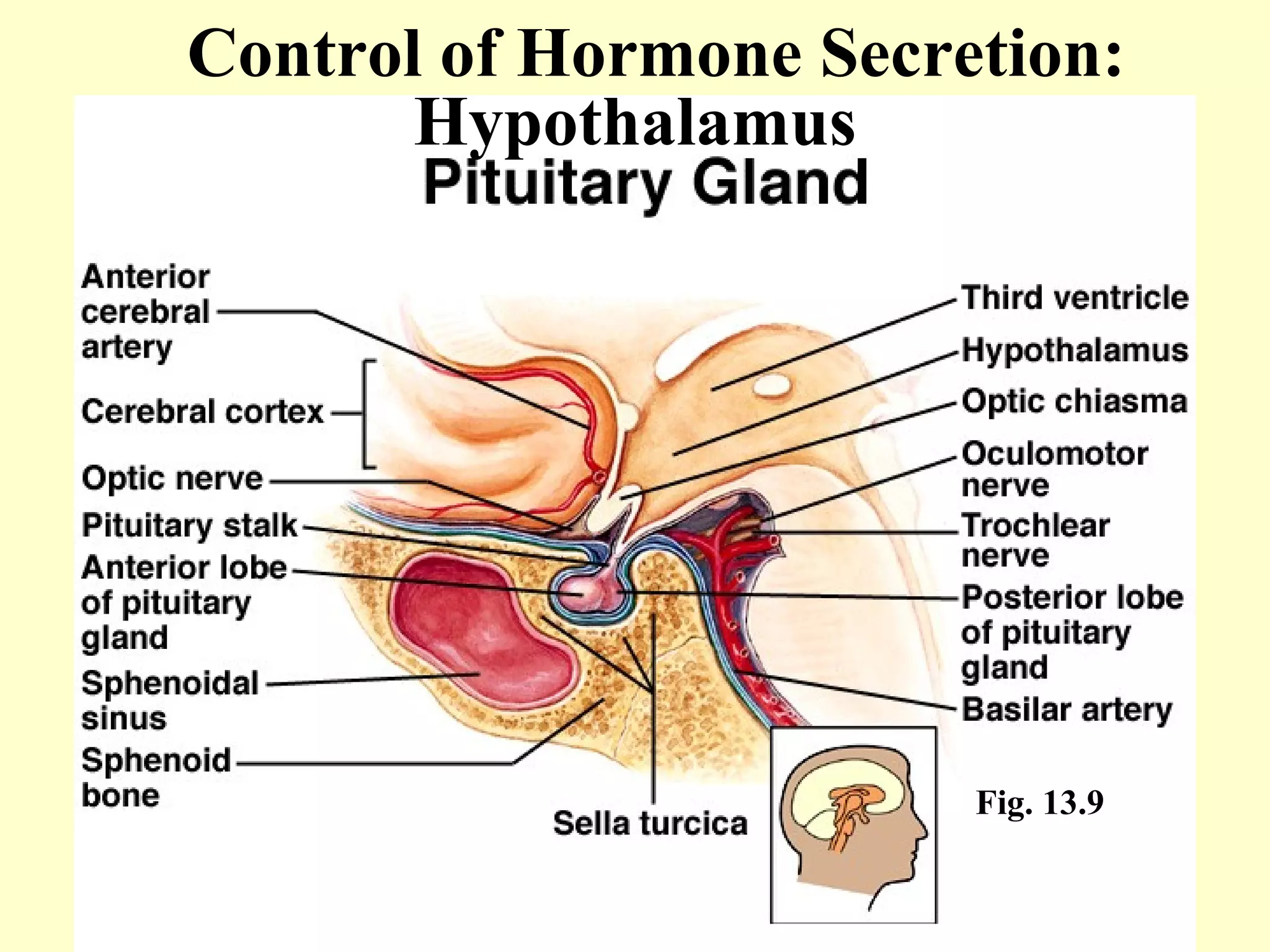
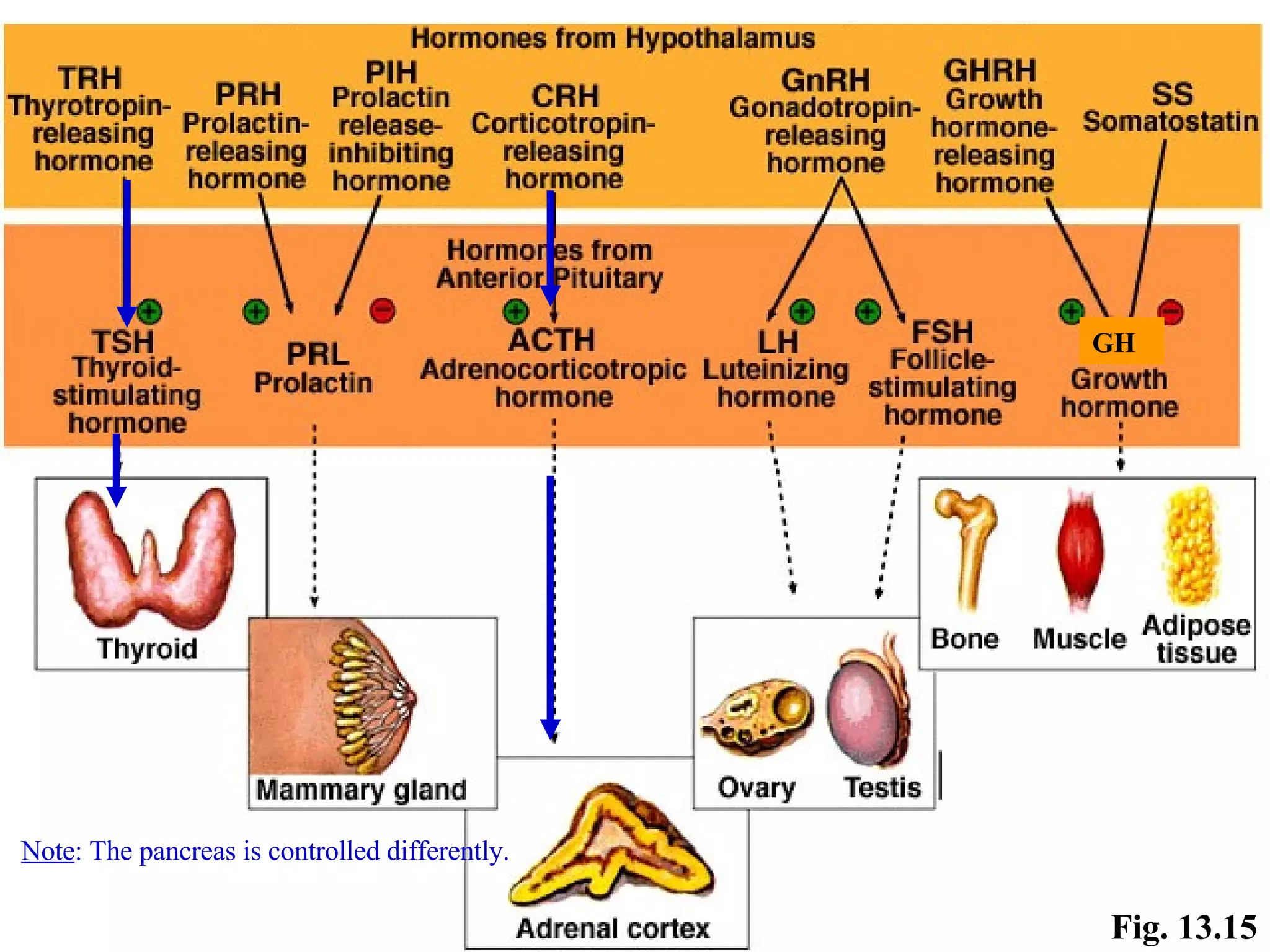
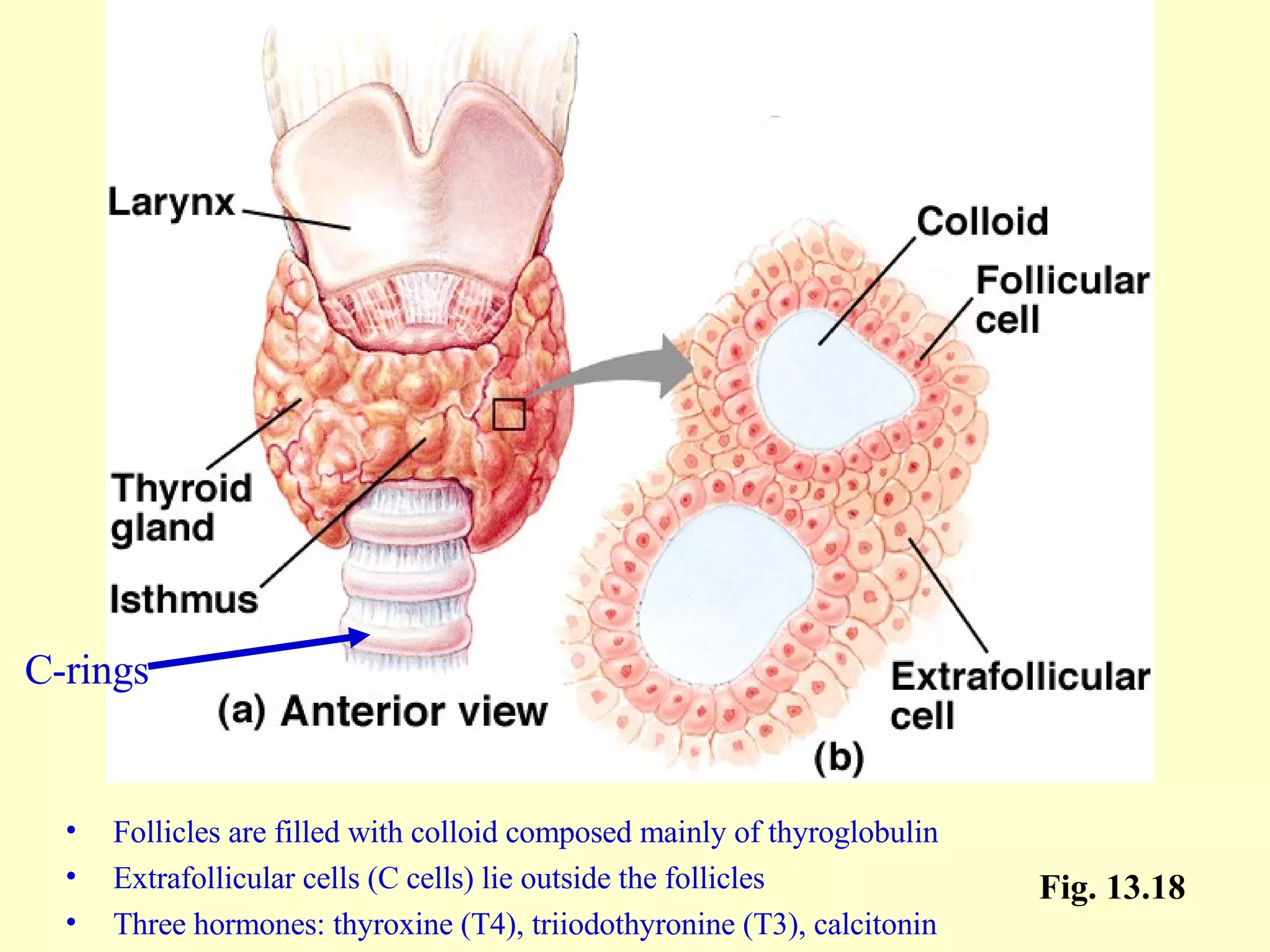
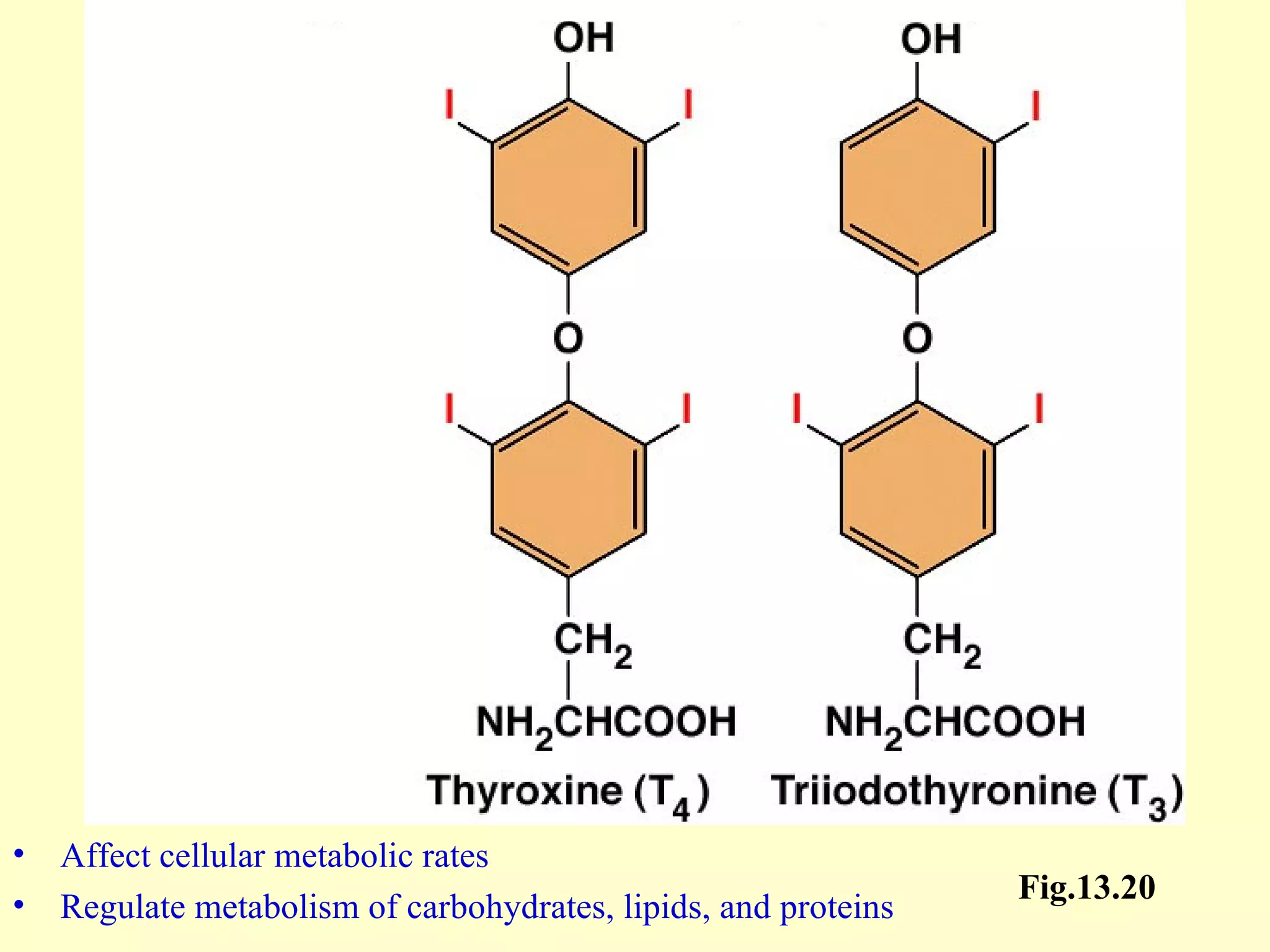
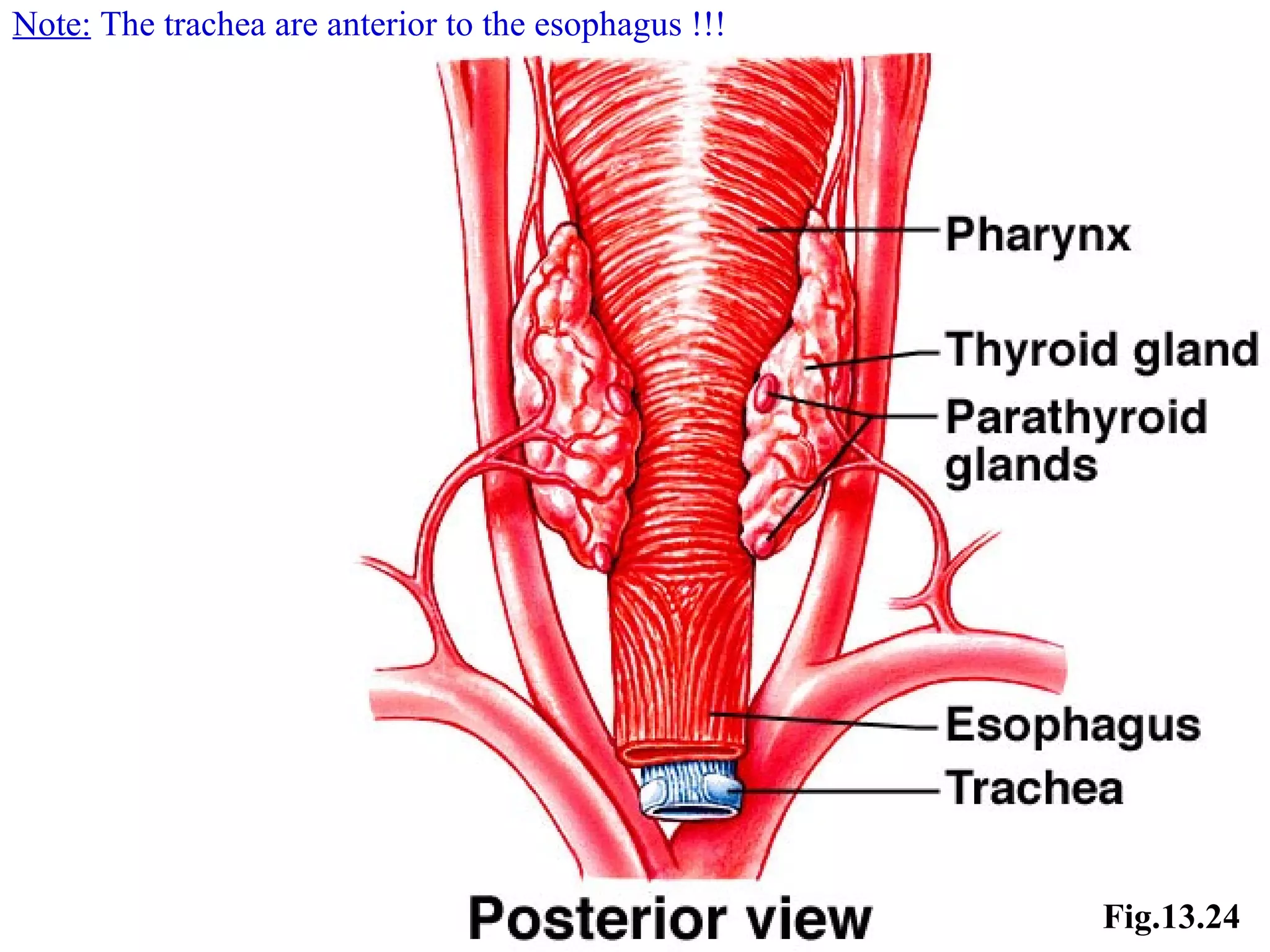
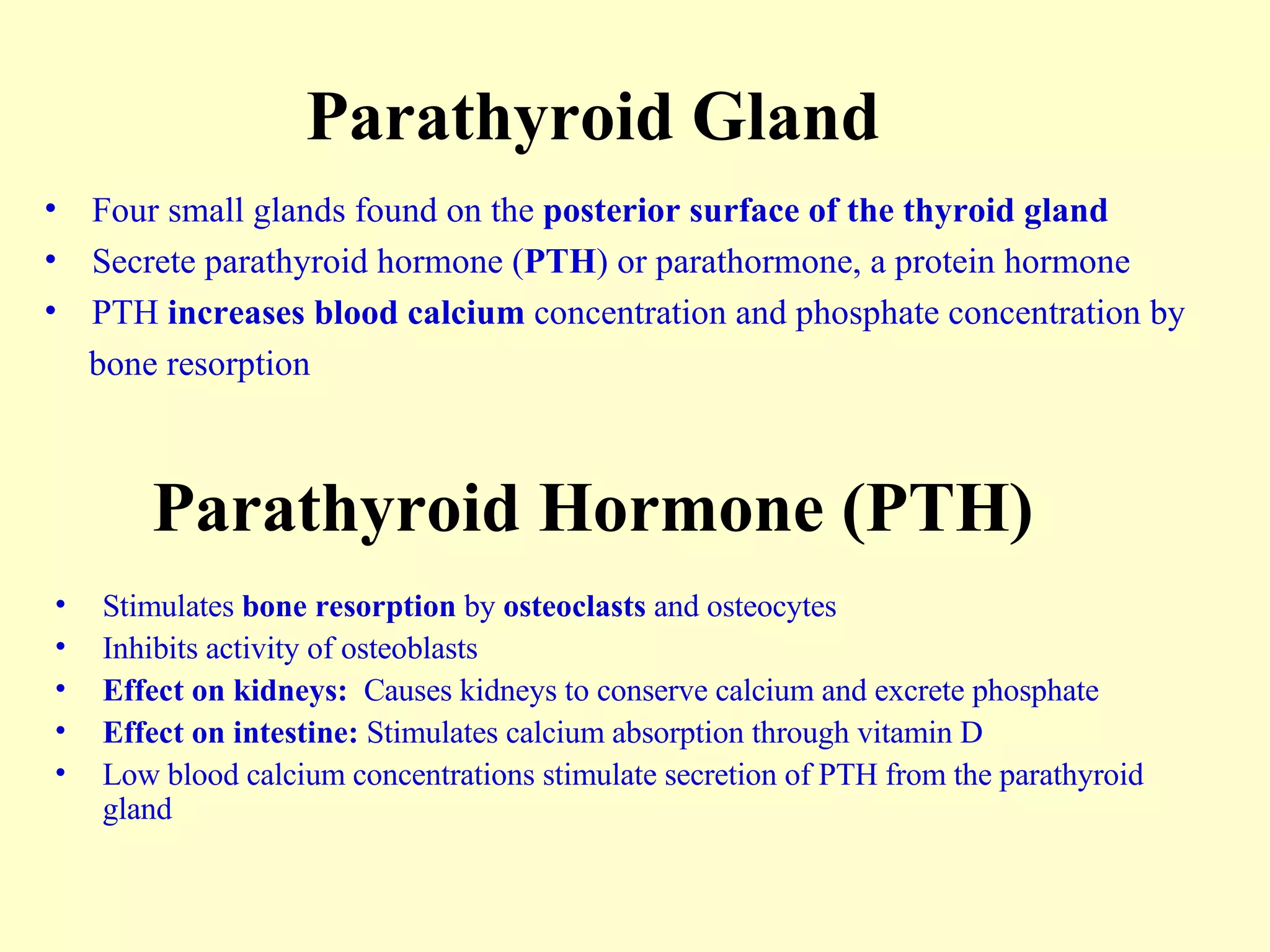
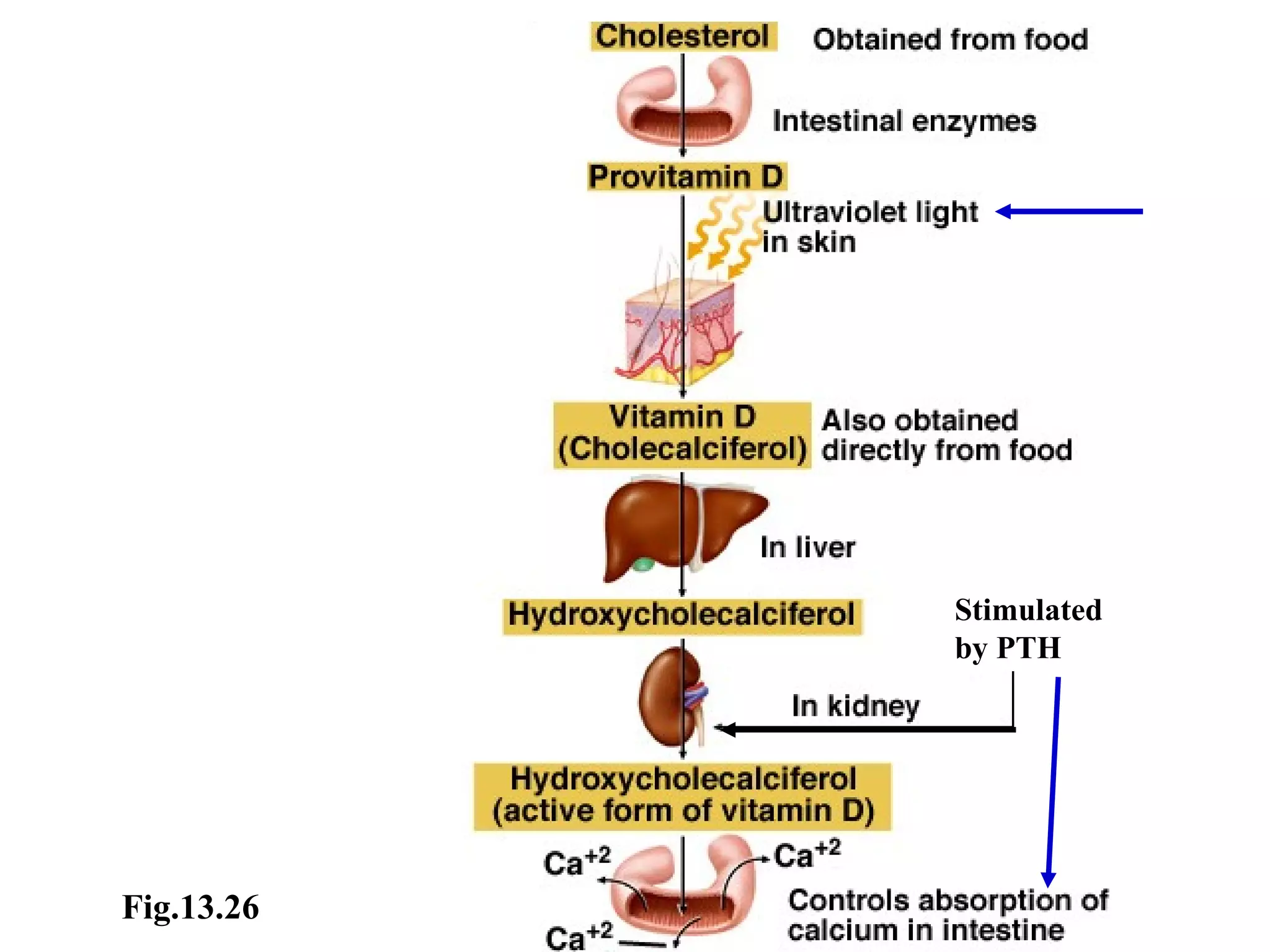
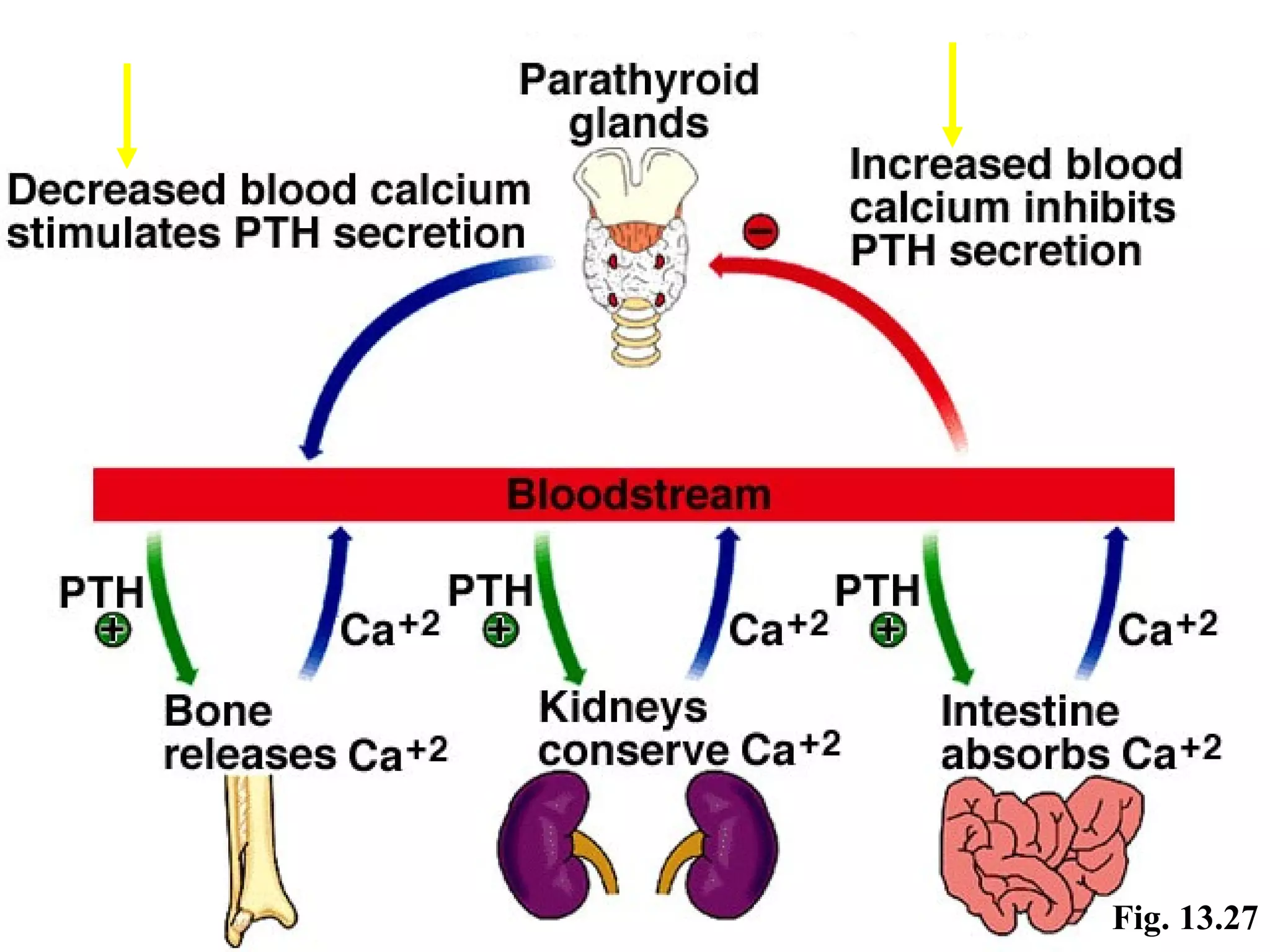
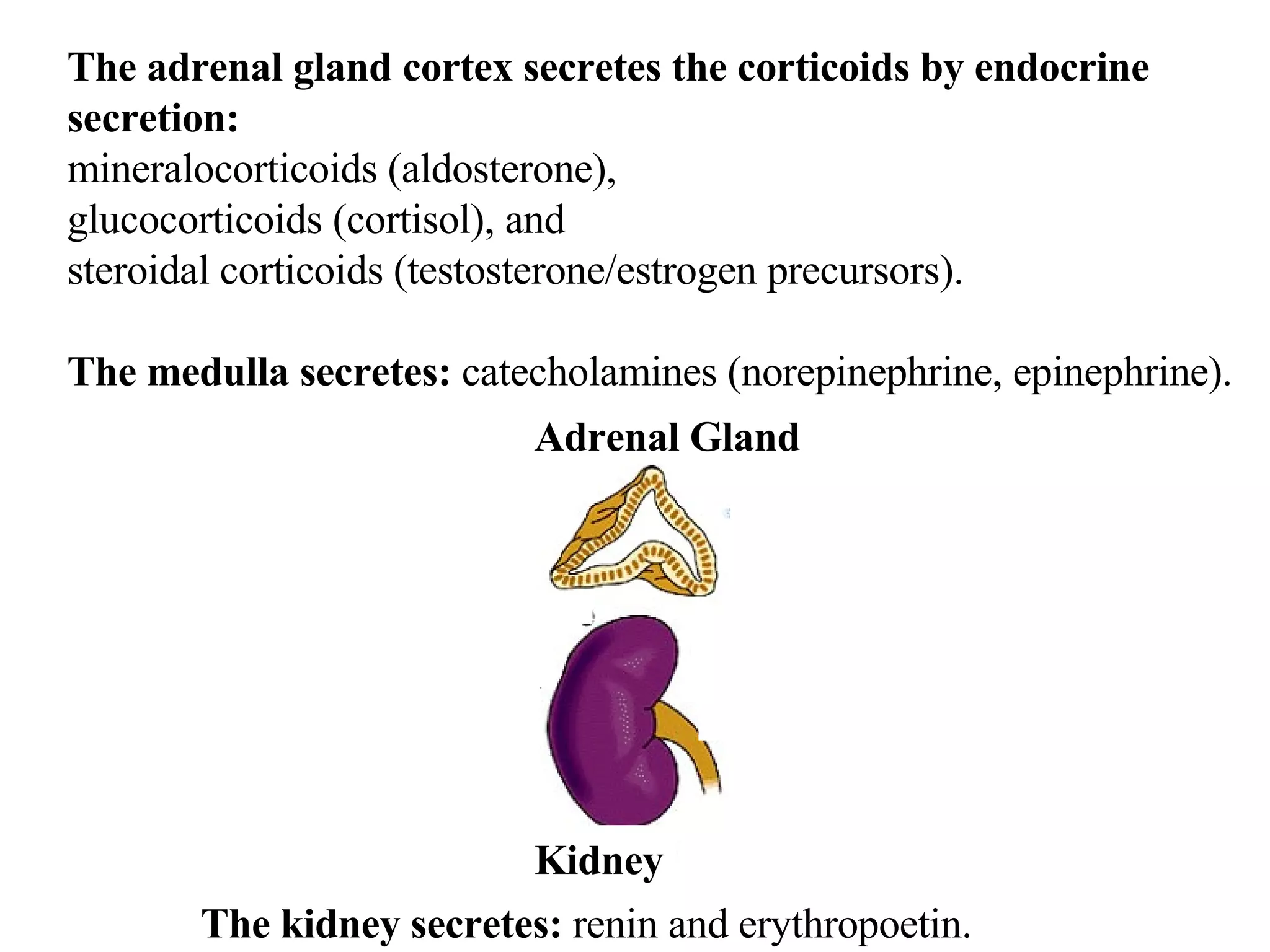
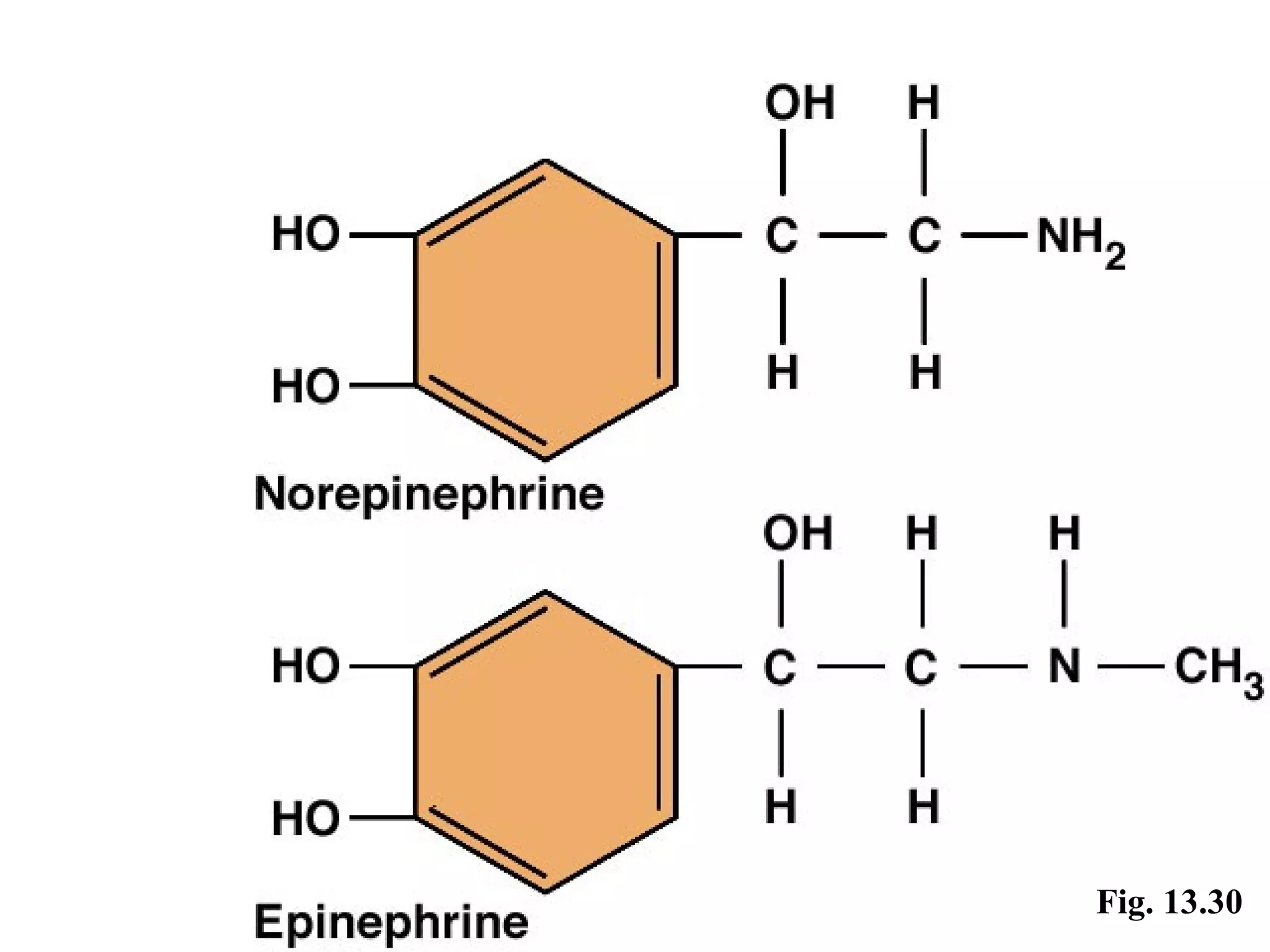
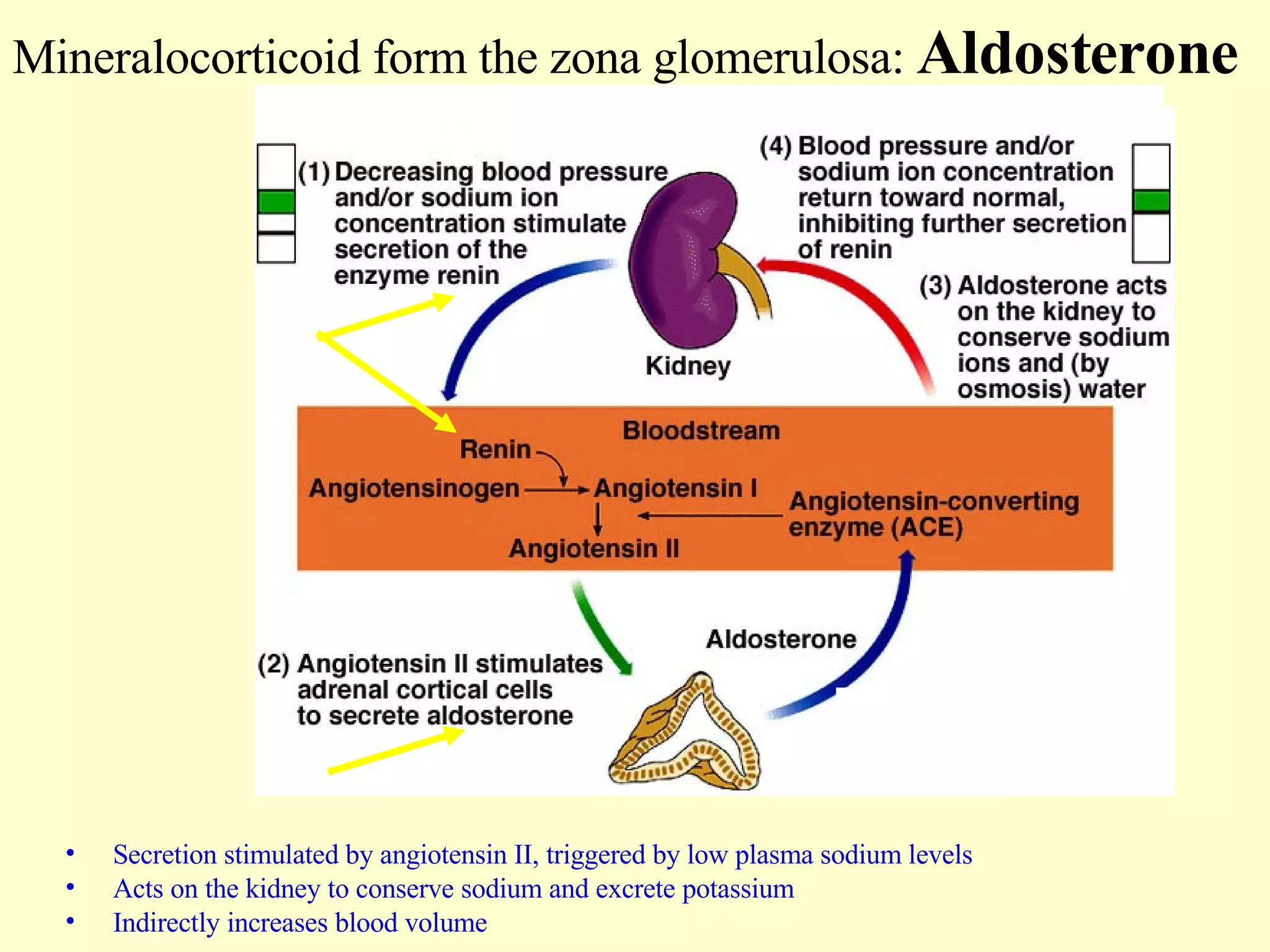
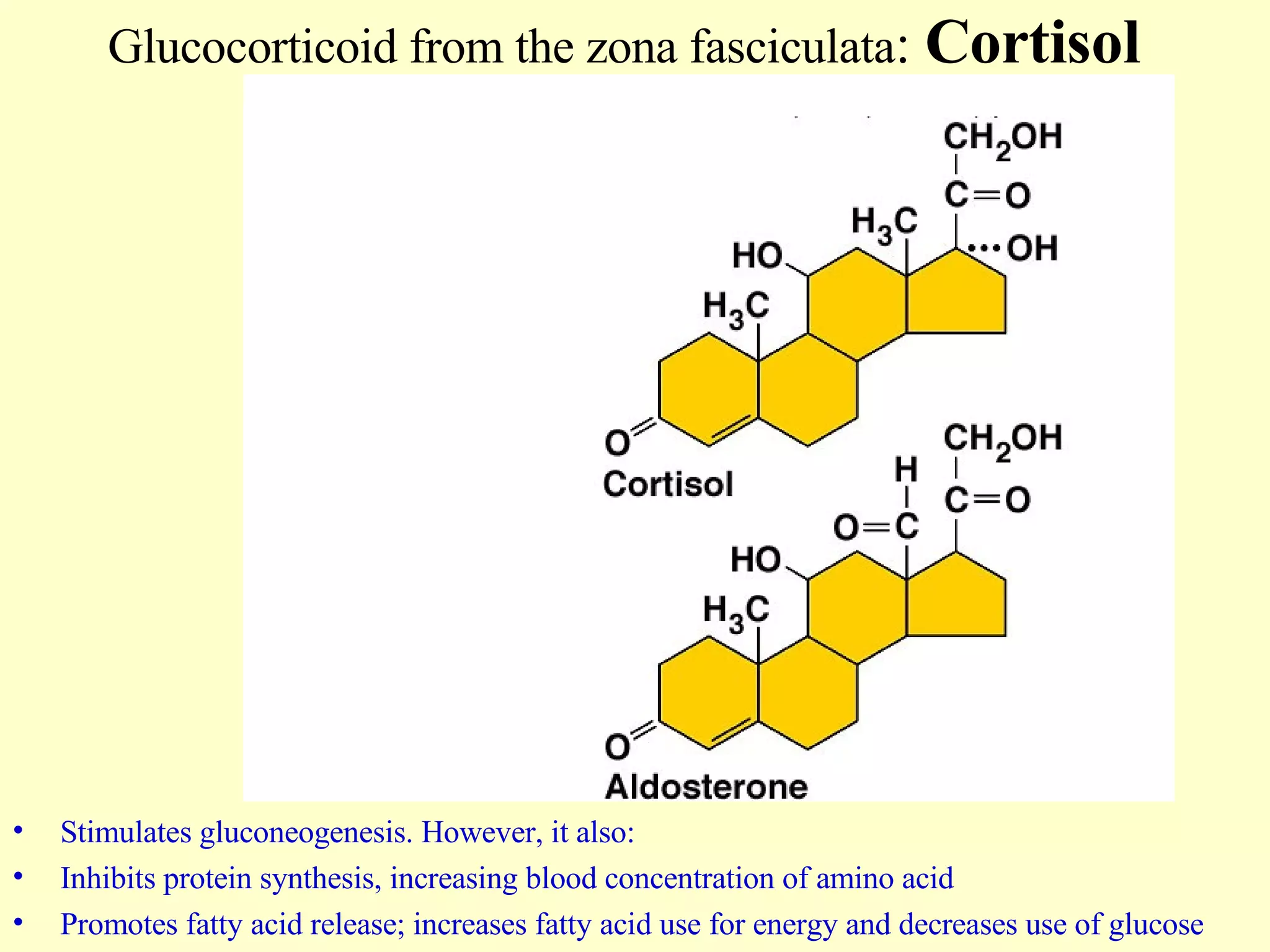
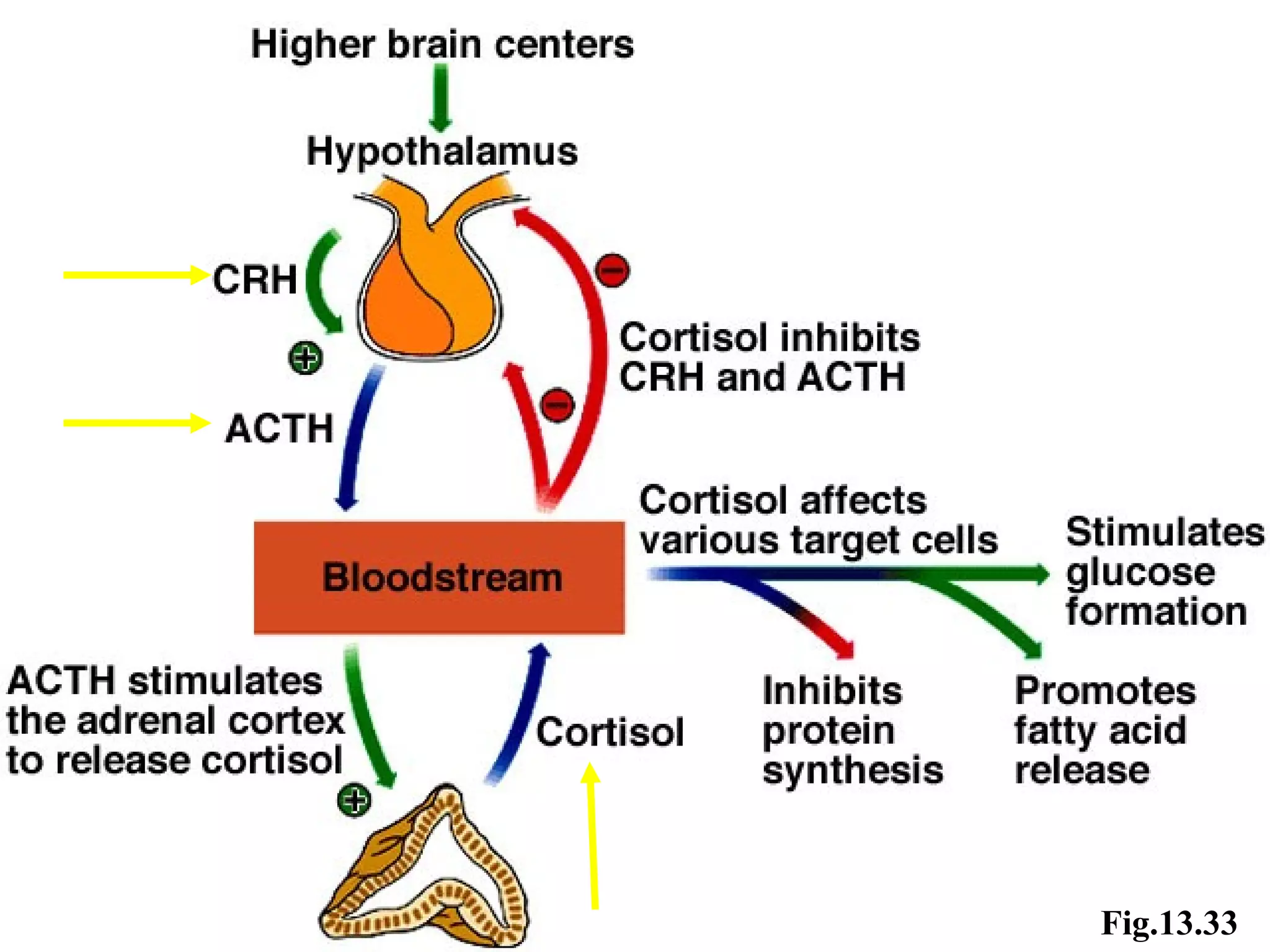
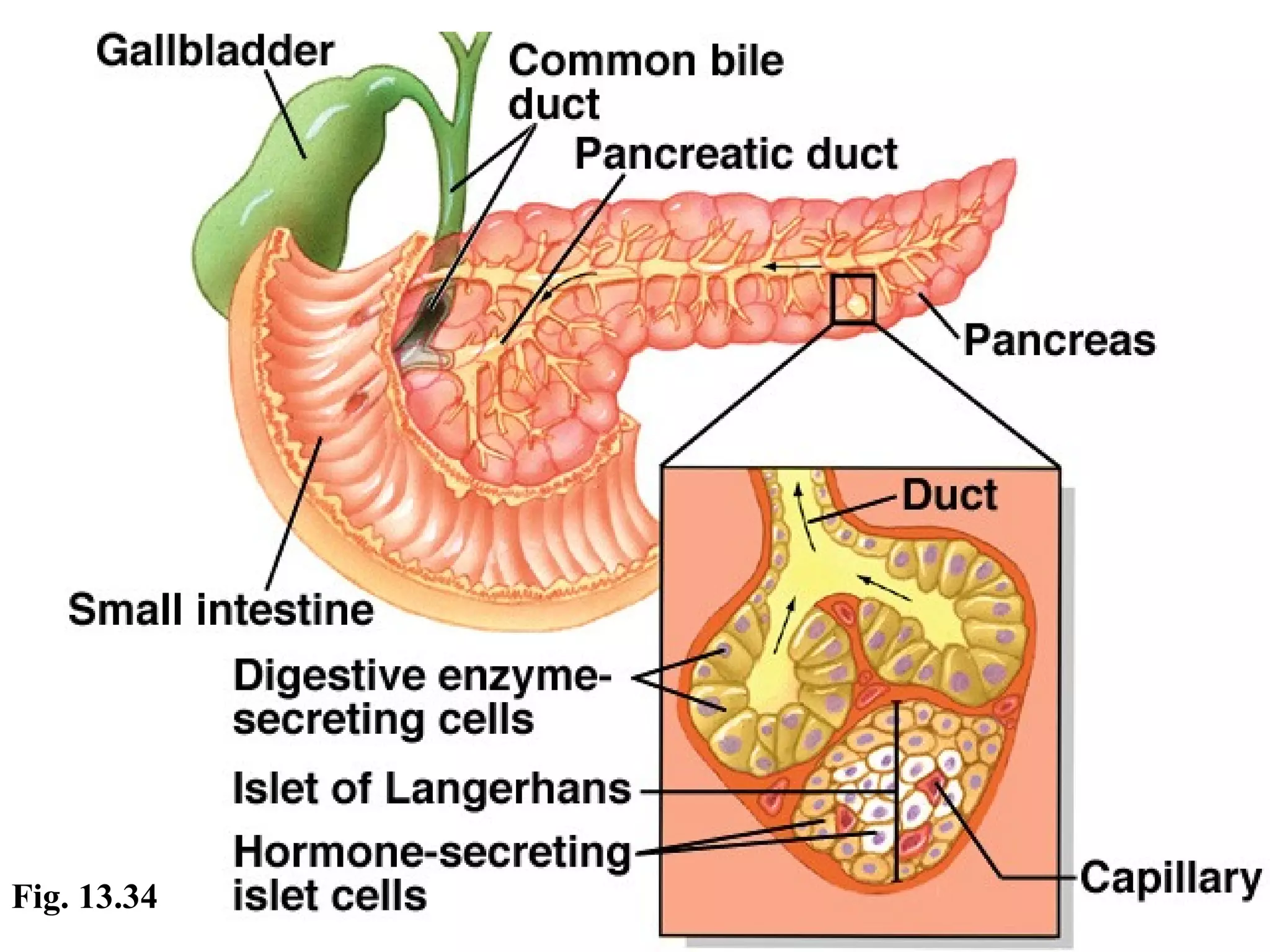
![You are responsible for the following figures and topics: Fig. 13.3 - Location of major endocrine glands. Fig. 13.9, 13.12, 13.13 – hypothalamus; pituitary gland. Fig. 13.4 - What are hormones ? Fig. 13.5, 13.7 - chemical structure predicts their mechanism of action. Fig. 13.11 - function of hormones is to keep balance / homeostasis. Read TB, p. 477. [see also: Fig. 13.16] Fig. 13.15 - Stimulation of anterior pituitary hormones by the releasing hormones of the hypothalamus. Read TB, p. 485, on thyroid gland. Fig. 13.18 - describe the location of the thyroid gland. Fig. 13.20 - describe 2 of the three thyroid hormones, T3 and T4. Tab. 13.7 - all 3 thyroid hormones: T3, T4, Calcitonin. Fig. 13.27 - PTH-parathyroid hormone Refer back to Ch.7 where we discussed osteoblasts and osteoclasts. Fig. 13.24 - Describe the structure, location and number of parathyroid glands. Figs. 13.21, 13.22, 13.23 - Define ' cretinism', 'hyperthyroidism' , 'goiter' Fig. 13.28 - Adrenal gland. Tab. 13.11 - Name the hormones and their function !!! Fig. 13.30 - Hormones released by the adrenal medulla. TB, p.492. Fig. 13.31 - Control of aldosterone, a mineralo-corticoid. Fig. 13.33 - Control of cortisol, a gluco-corticoid. Read TB, p.496, on the pancreas. Fig. 13.34 - Describe the location of the pancreas. Tab. 13.12 - Describe the function of glucagon. Clinical Application 13.4 - IDDM Read TB, p.498, pineal gland. TB, p.500 - other hormones of interest.](https://image.slidesharecdn.com/the-endocrine-system-1203747098311455-2/75/The-Endocrine-System-Chapter-13-2-2048.jpg)
![HOMEOSTATIC IMBALANCES (i.e. abnormal hormonal levels) A. Diabetes Mellitus [introduction, p.468; Clin. Appl. 13.4, p.499] Symptoms (3 poly's): polyuria, polydypsia, polyphagia . Type I /IDDM (10%) – insulin-deficiency: autoimmune disorder where β-cells are destroyed; absolute insulin deficiency, with insulin administration. Patients < 20 years; - results in Hyperglycemia Cells can't use glucose=fat is broken down, releasing ketone bodies, causing ketoacidosis, lowering blood pH, causing death. Complications include Atherosclerosis, CV disease, IHD, PVD, gangrene, blindness due to cataracts (lens) and retinal vascular disease; renal failure. Treatments: artificial pancreas that detects fall in glucose levels and automatically releases insulin; transplant of pancreas or Beta cells. b. Type II /NIDDM (90%) – non-insulin-deficient, but receptor deficient: patients > 40 years, overweight, hypertension, hyperglycemia Problem is usually with the loss of receptors on target cells; Controlled by diet, exercise, and weight loss; Treatment: Drug Diabeta (glyburide): to help stimulate insulin secretion of β-cells in cases of low levels of insulin .](https://image.slidesharecdn.com/the-endocrine-system-1203747098311455-2/75/The-Endocrine-System-Chapter-13-46-2048.jpg)
















































































![Coded Agents – with UiPath SDK + LangGraph [Virtual Hands-on Workshop]](https://cdn.slidesharecdn.com/ss_thumbnails/codedagentsdeck-251215155422-5497c599-thumbnail.jpg?width=640&height=640&fit=bounds)






