Downloaded 213 times
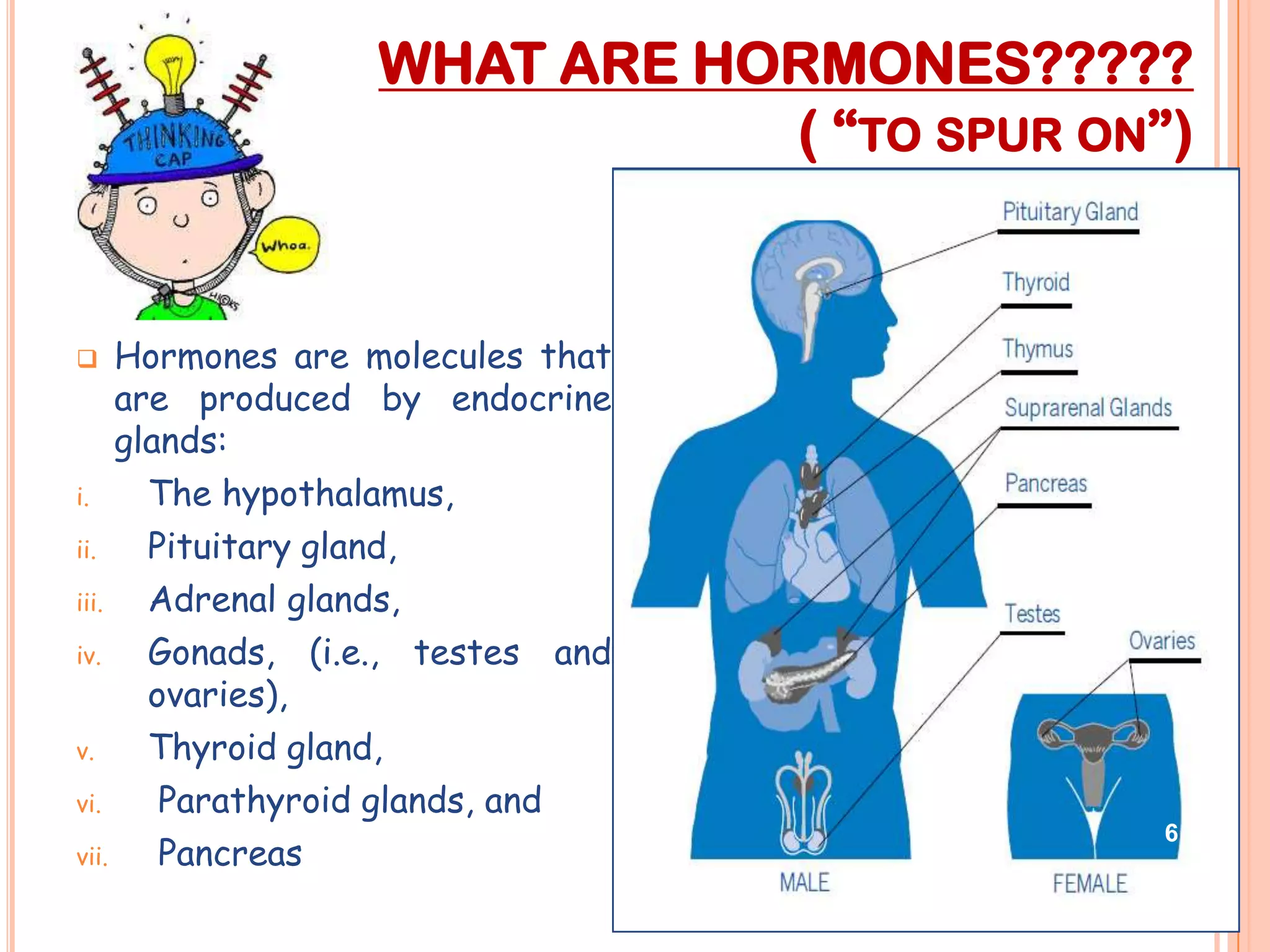
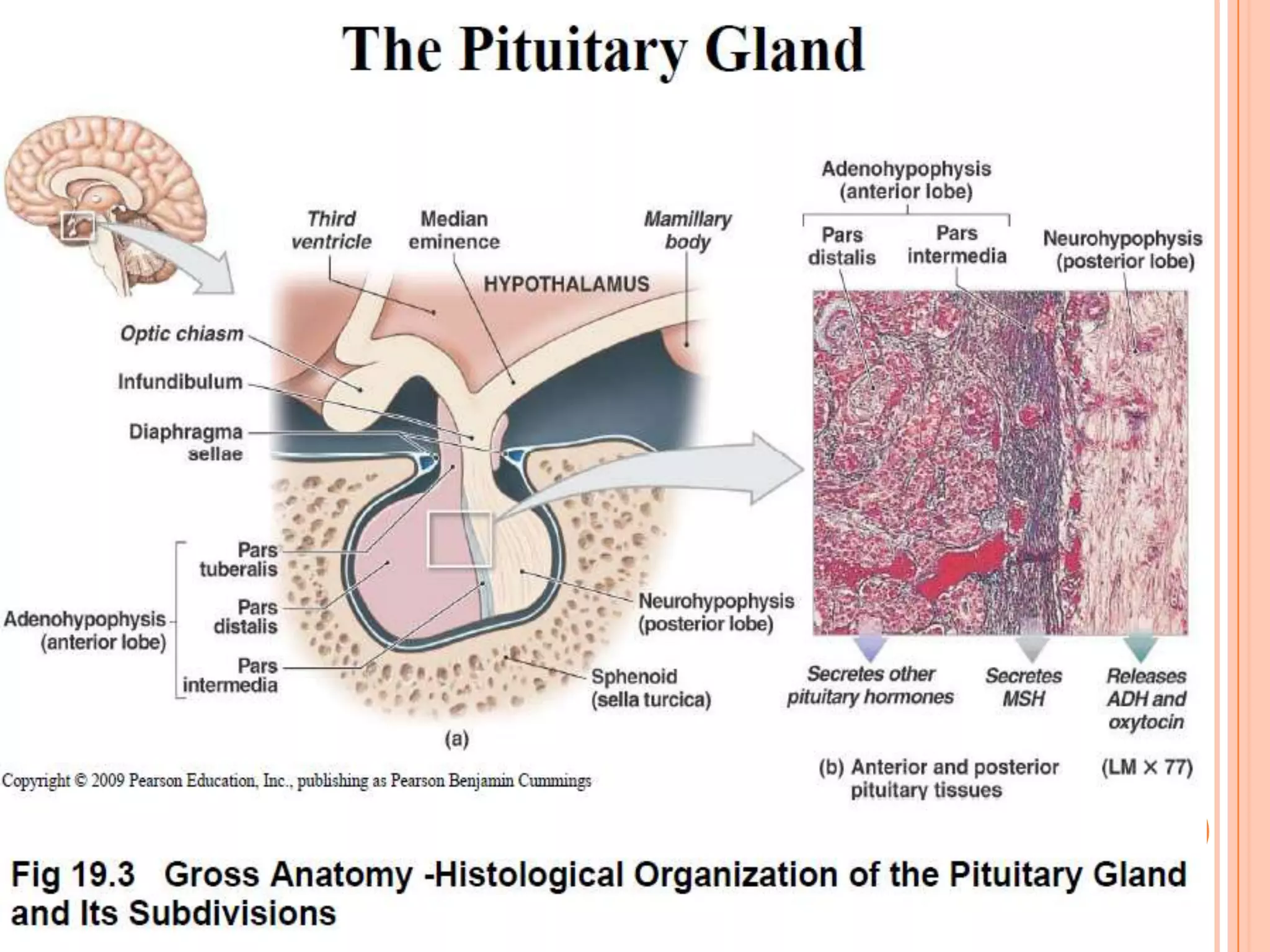
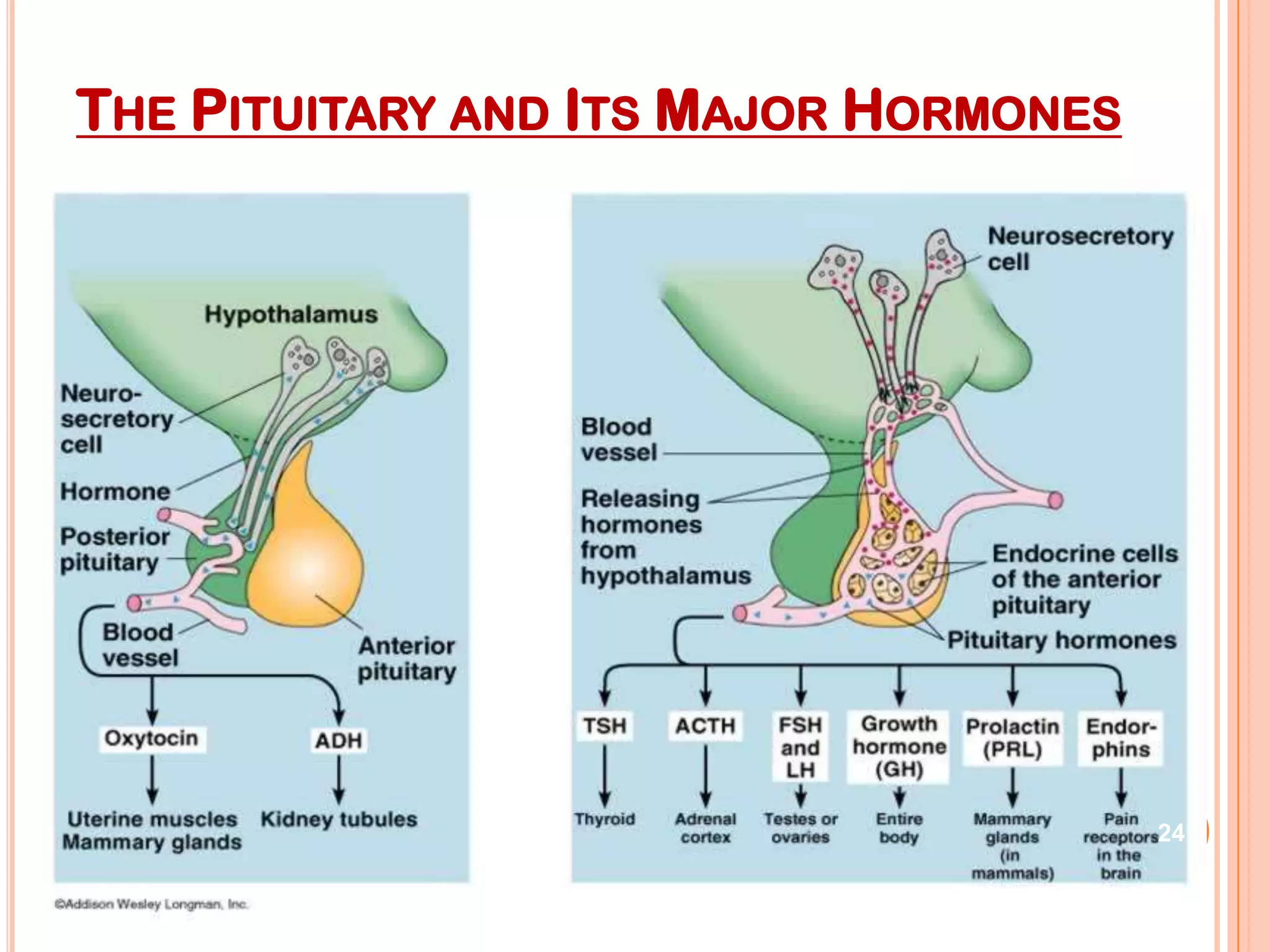
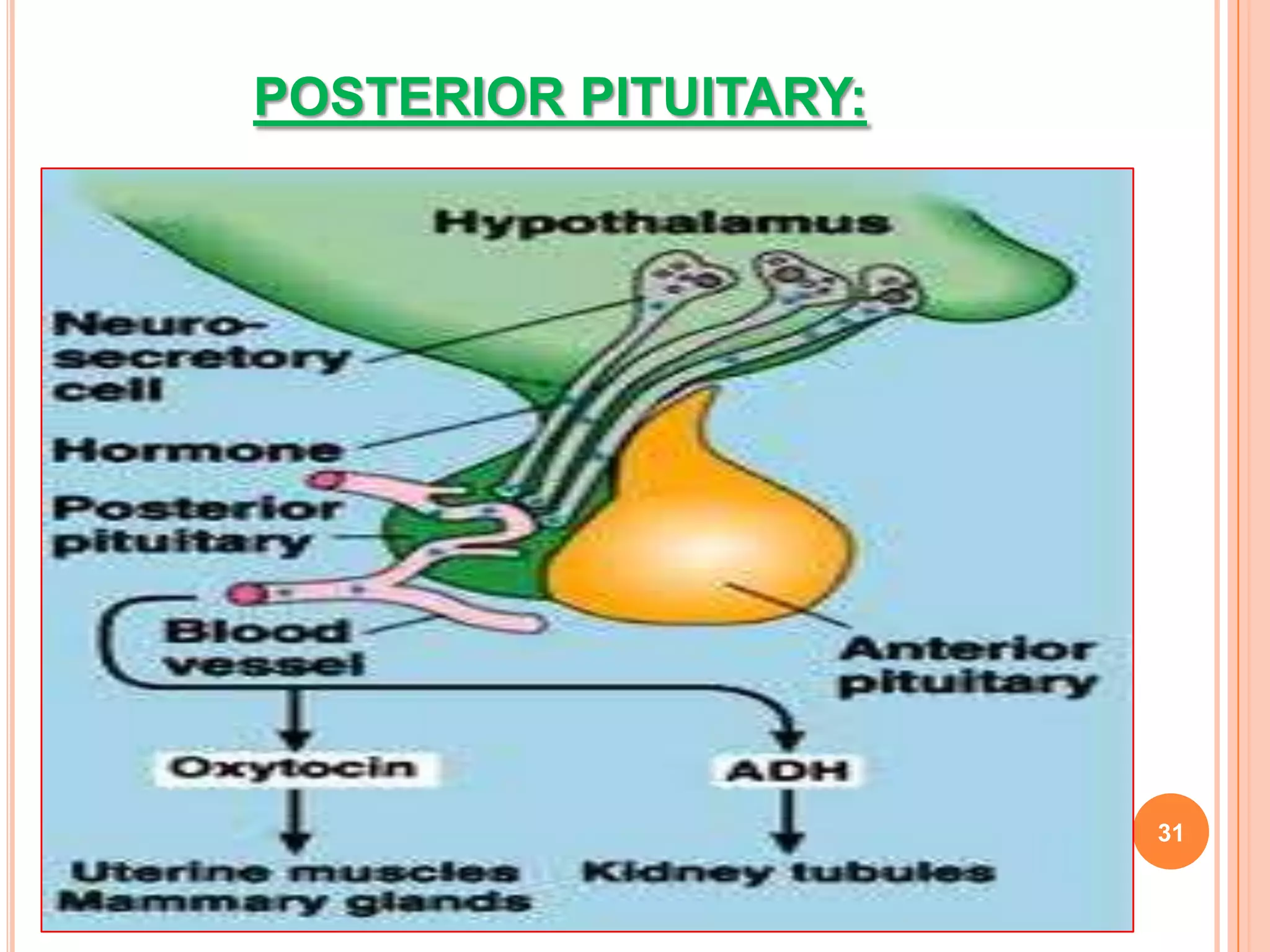
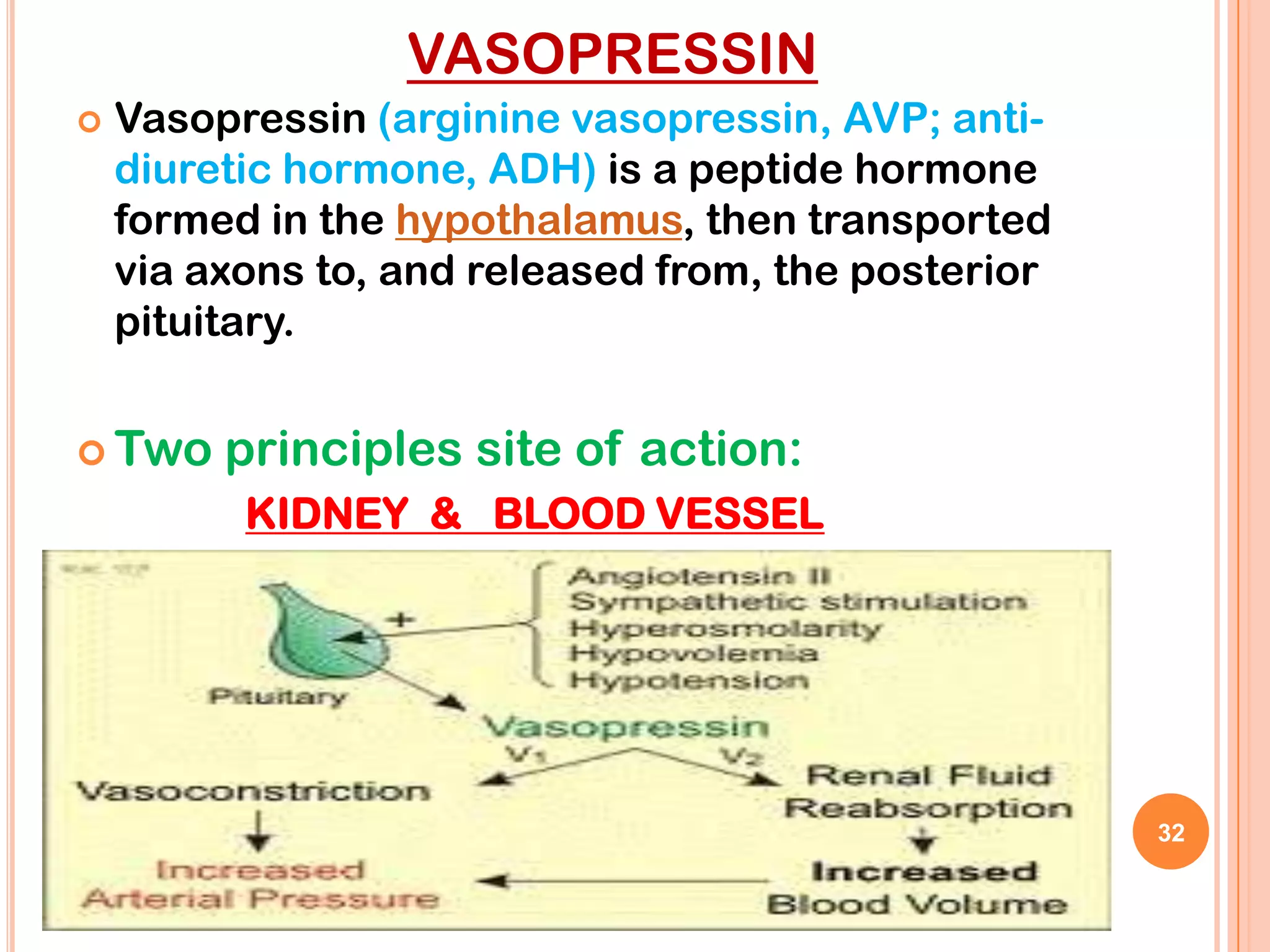
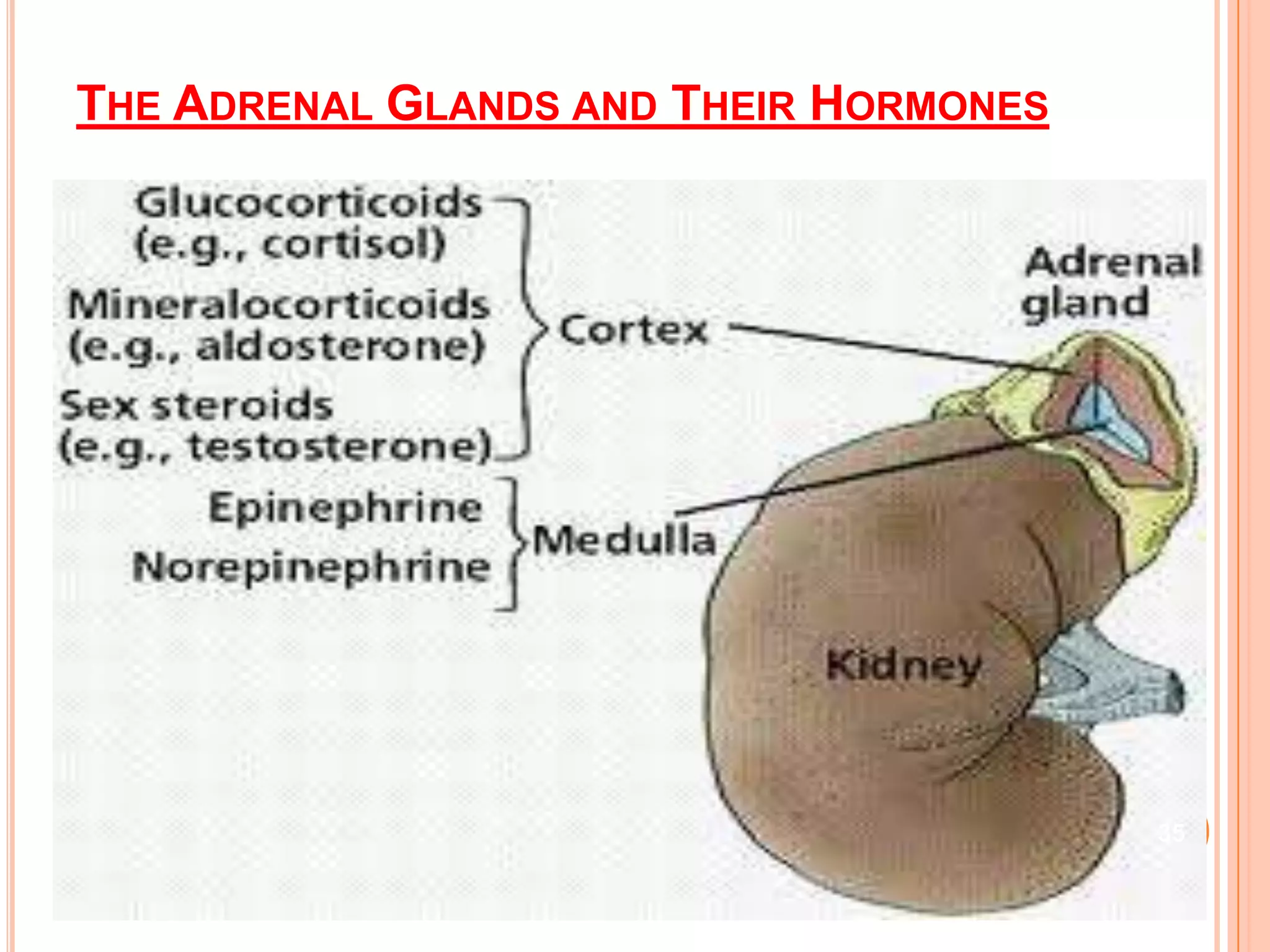
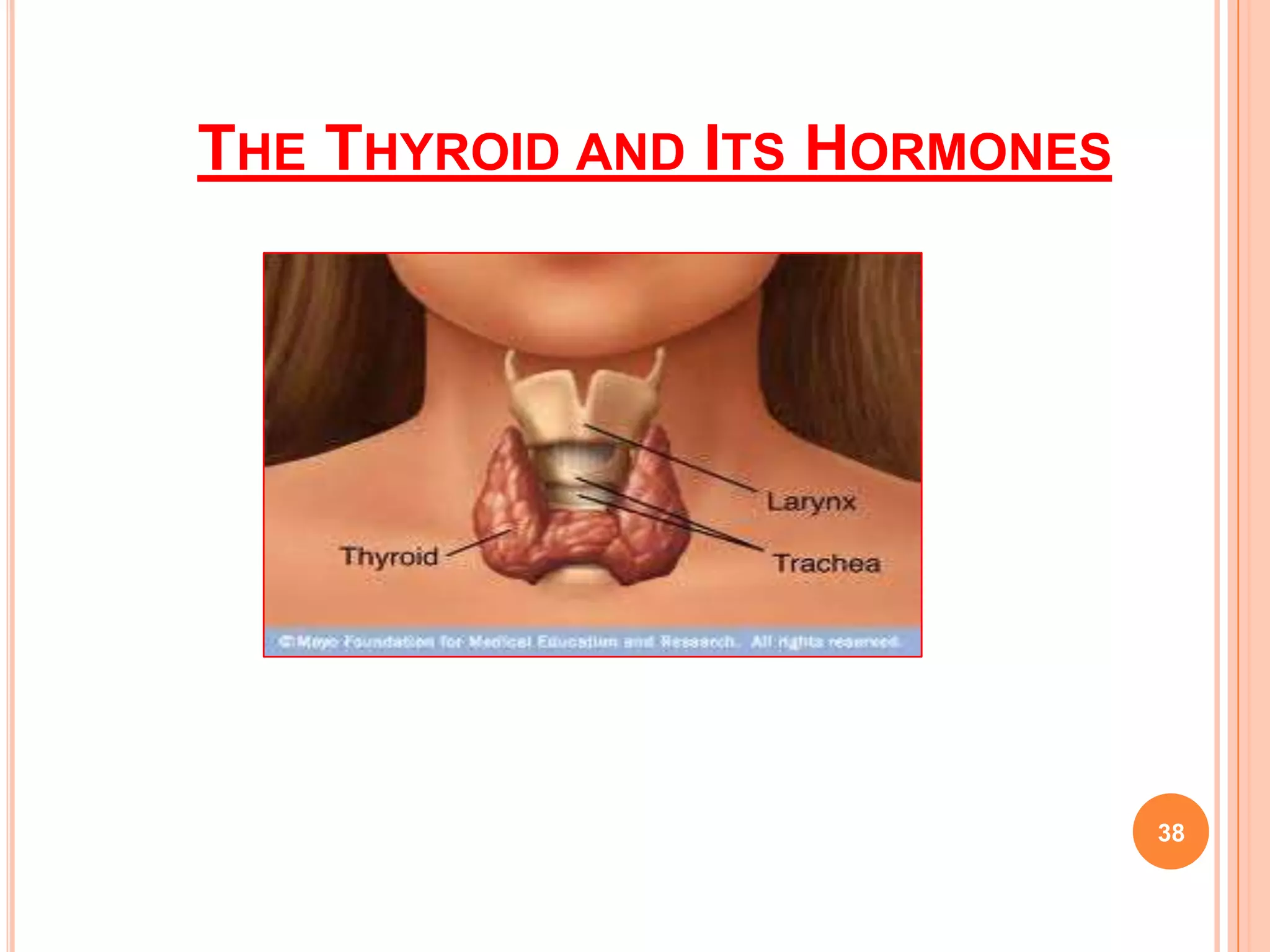
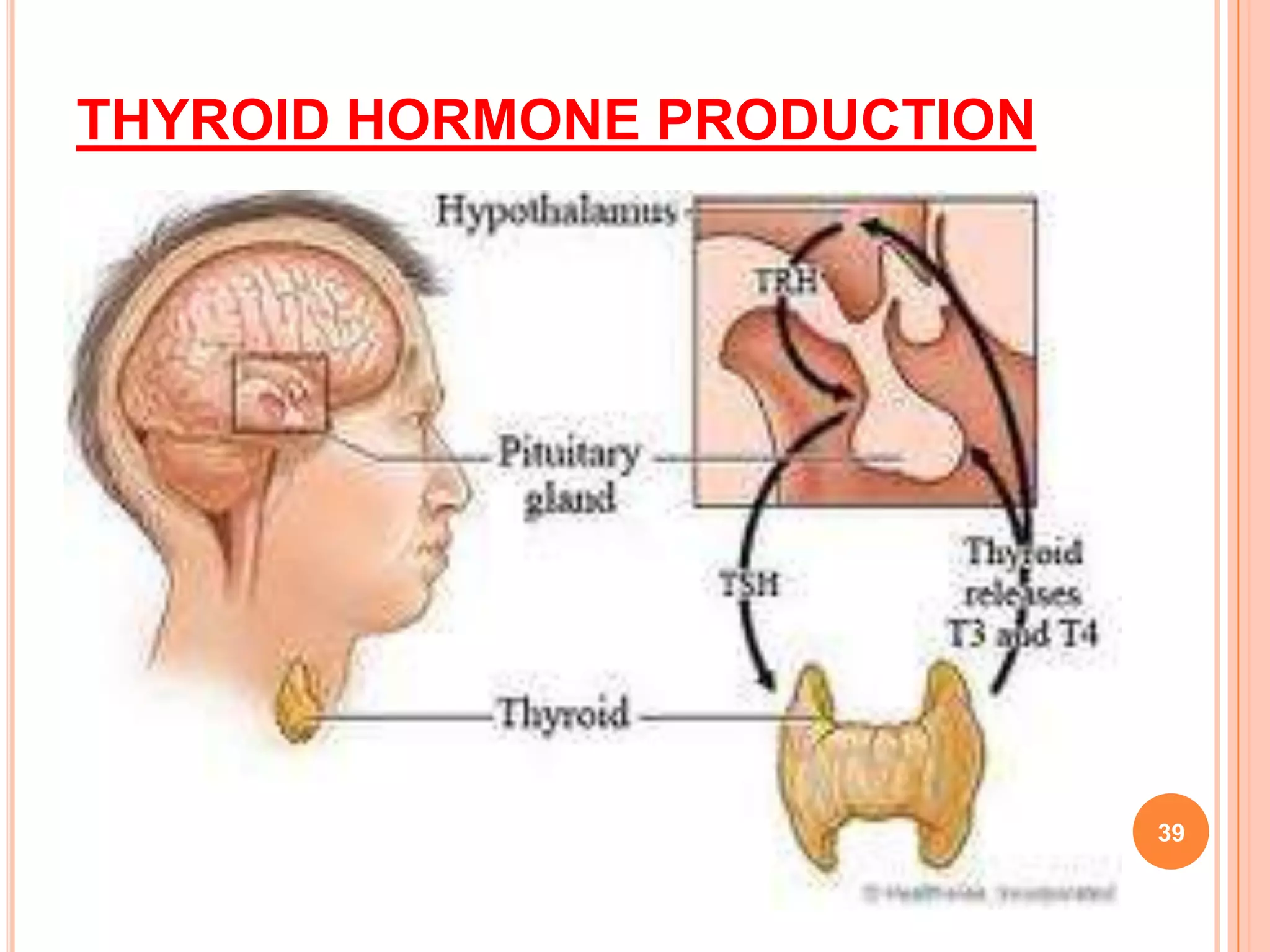
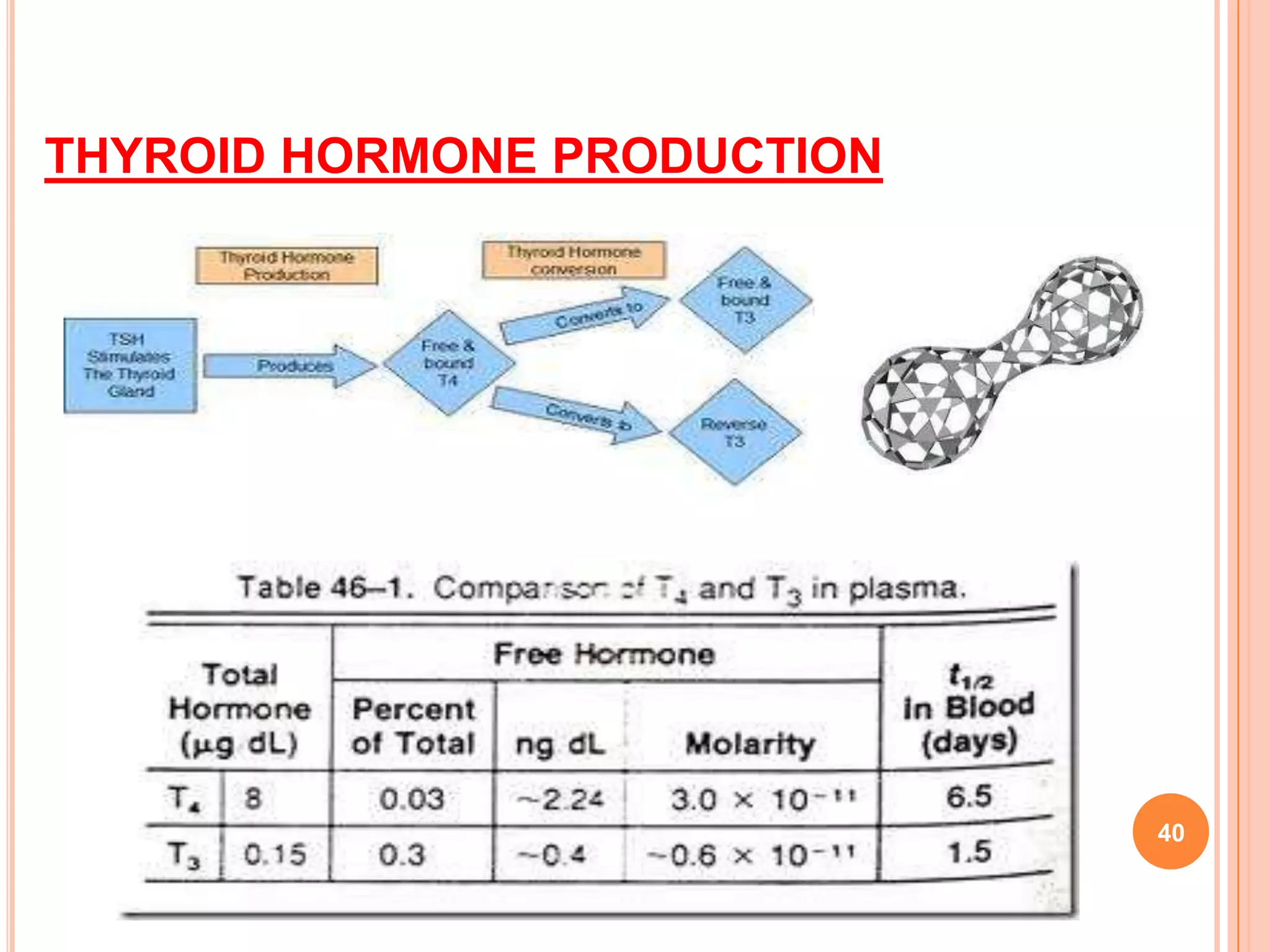
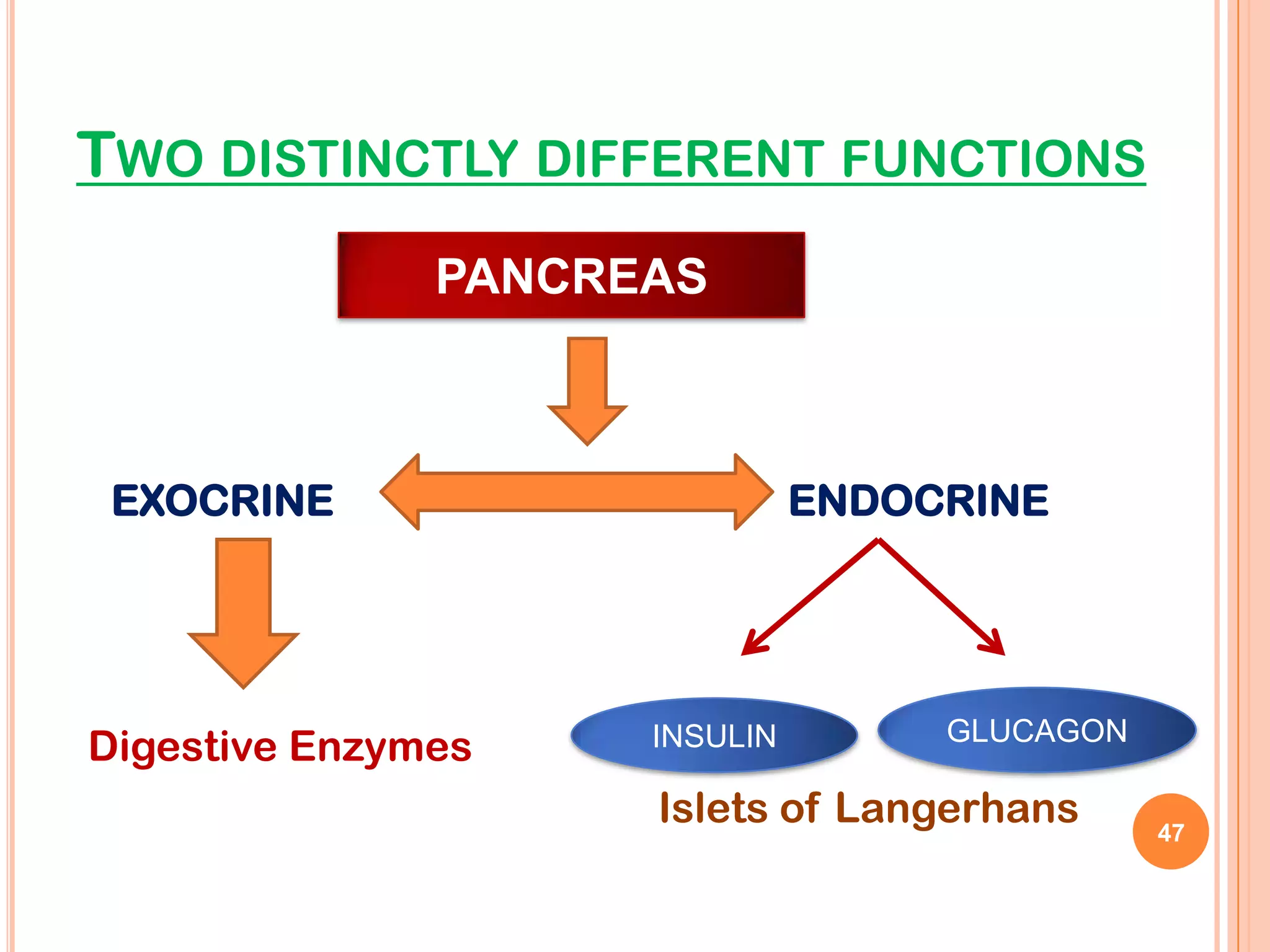
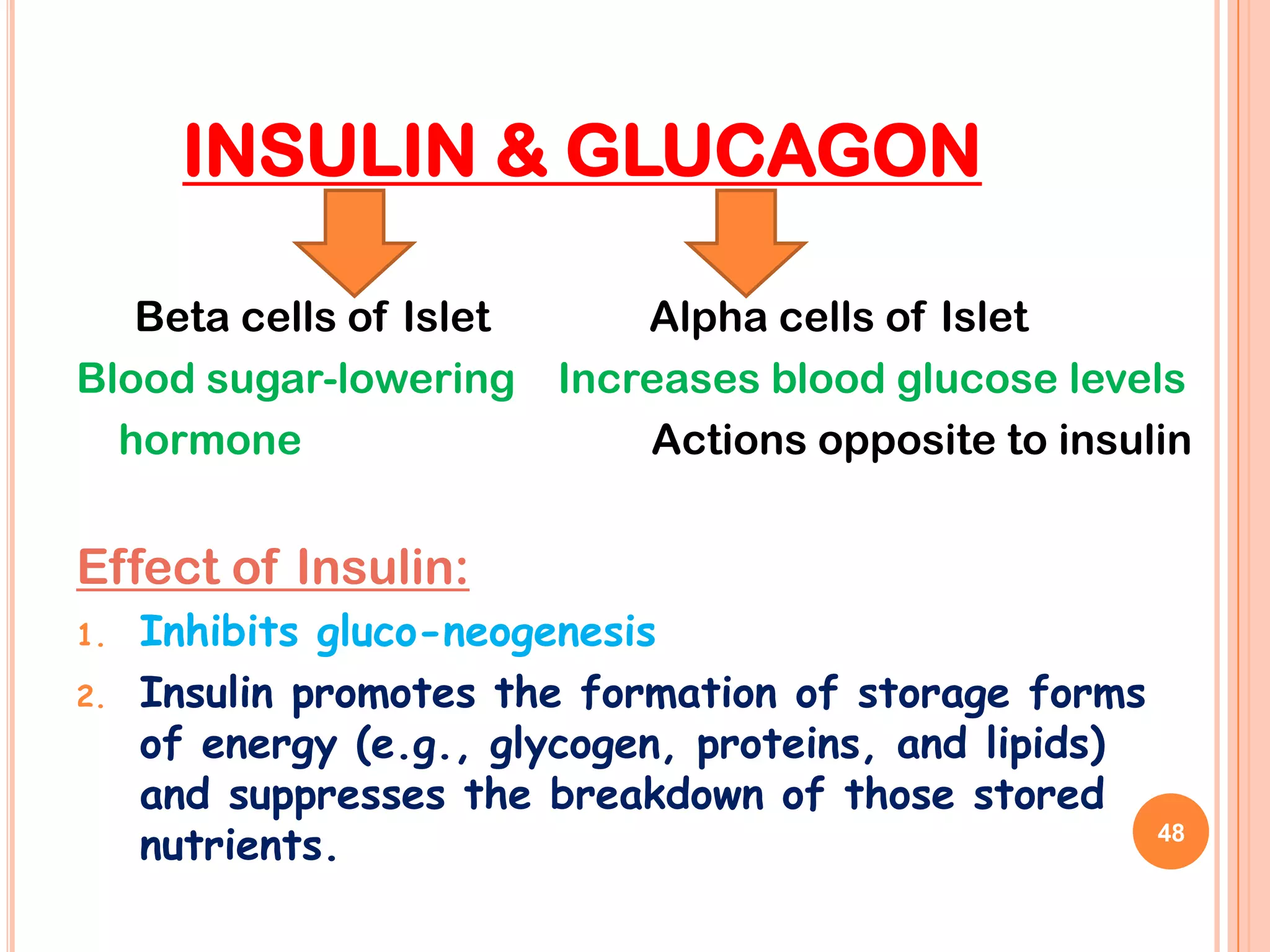
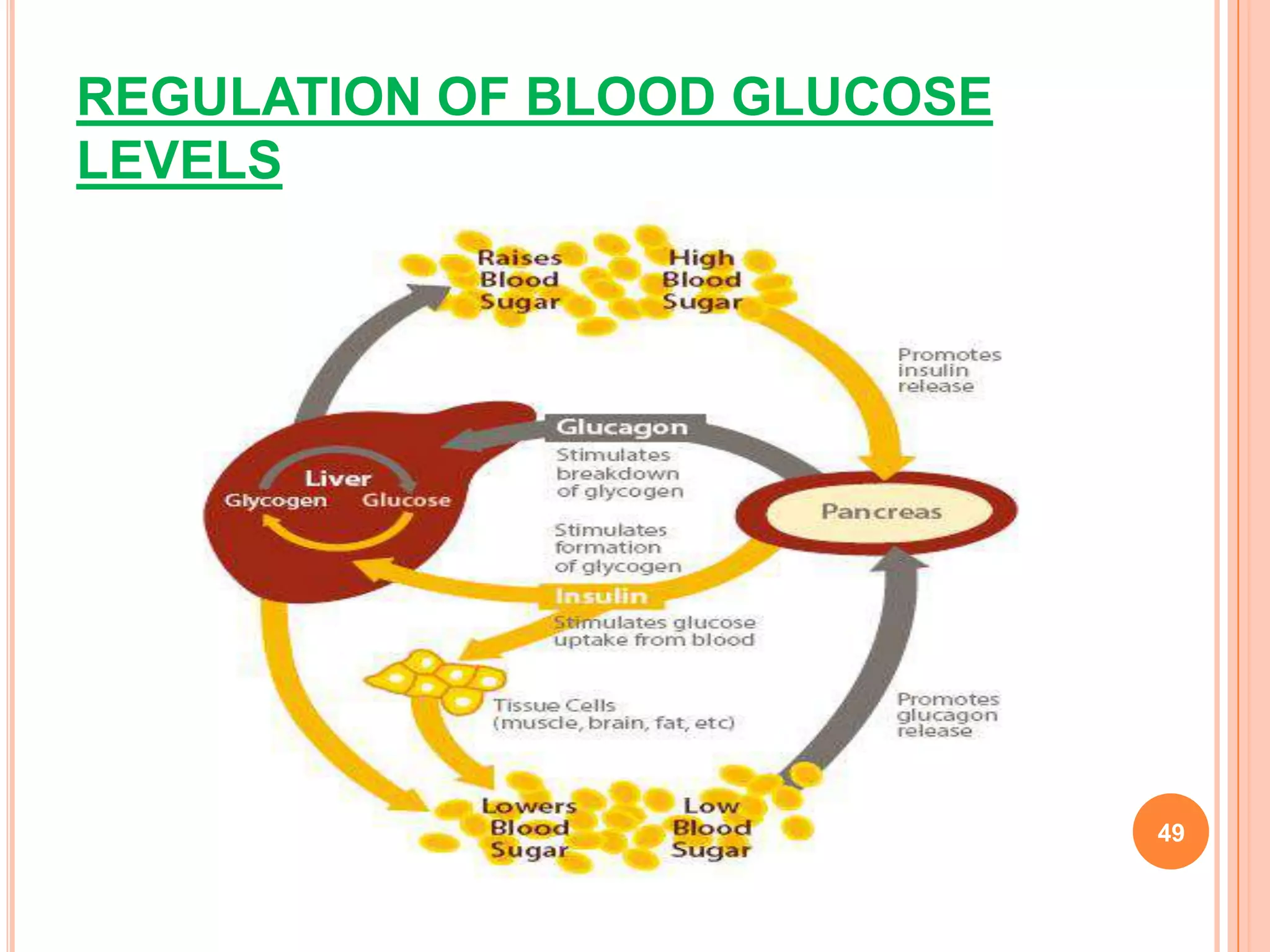

The document discusses the endocrine system, describing the major glands including the hypothalamus, pituitary gland, thyroid gland, parathyroid glands, adrenal glands, pancreas, and gonads. It explains the hormones produced by each gland and their roles in regulating processes like growth and development, metabolism, fluid balance, and reproduction. Common endocrine disorders in children like diabetes are also mentioned.