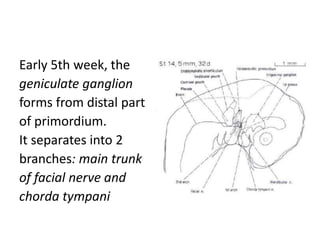
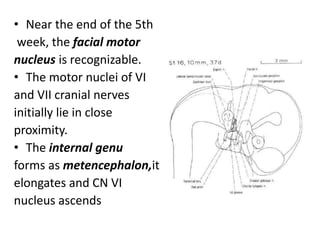
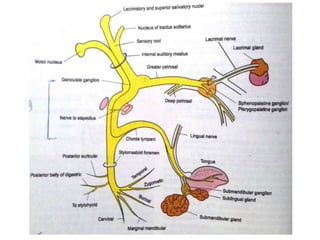
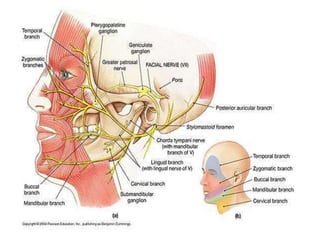
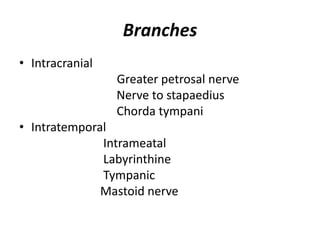
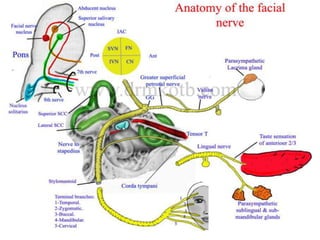
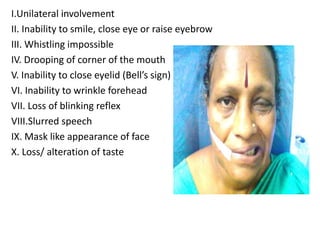
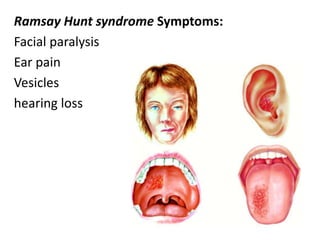


The document provides a comprehensive overview of the facial nerve, including its embryology, anatomical course, branches, functional components, and clinical considerations. The facial nerve controls muscles of facial expression, conveys taste sensations, and interacts with several head and neck ganglia. It discusses variations, testing methods, and potential surgical implications related to the facial nerve.



































































