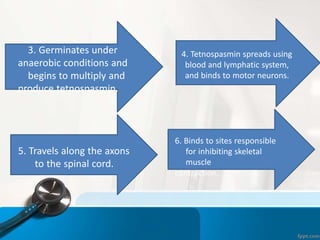
Tetanus is caused by Clostridium tetani bacteria. It causes painful muscle spasms and rigidity. The bacteria enters through wounds and releases a toxin that binds to motor neurons. This causes prolonged muscle contractions. Symptoms include lockjaw, arching of the back, and muscle spasms. Diagnosis is clinical based on symptoms. Treatment involves wound cleaning, antibiotics, muscle relaxants, and immunoglobulins to neutralize toxins. Prevention through regular tetanus vaccination is highly effective.