Increase atrial and ventricular mA
6. AAI: normal atrial pacing
7. VVI: normal ventricular pacing
8. DDD: failure to sense atria; increase atrial sensitivity
9. DDD: failure to capture ventricle; increase ventricular mA
Temporary pacemakers
Objectives
– Defination
–Explain the situations when temporary
pacemakers are indicated.
– Describe the principles of pacing.
– Illustrate normal and abnormal pacemaker
behavior.
– Discuss the steps to be taken in troubleshooting
a temporary pacemaker.
2
3.
Definition
• Cardiac Pacemaker:is a medical device that
generates electrical impulses delivered by electrodes
to cause the heart muscle chambers to contract and
therefore pump blood.
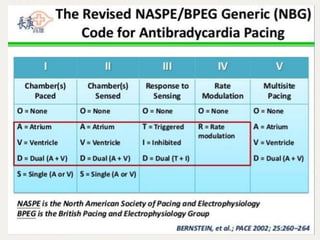
• T-Triggered: The pacemaker will pace in response to
sensed event.
• I-Inhibited: The pacemaker will not pace if it senses
an intrinsic event.
3
4.
Indications for TemporaryPacing
• Bradyarrhythmias
• AV conduction block
– Congenital complete heart block (CHB)
• L-Transposition (corrected transposition)
• Surgical/ cardiac interventions
• Trauma
• Slow sinus or junctional rhythm
• Permanent pacer malfunction
• Drugs, electrolyte imbalances
• Sick Sinus Syndrome
– Secondary to pronounced atrial stretch
– Old TGA s/p Senning or Mustard procedure
4
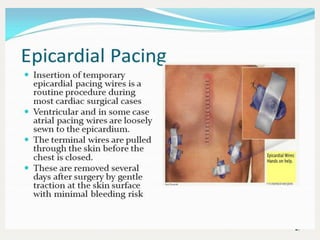
Epicardial Pacing
• Themost common method of temporary pacing
in cardiac ICU via postoperative epicardial wires
• A pair of Wires sutured to right atrium & right
ventricle epicardium.
• Atrial wires exit on the right of the sternum
• Ventricular wires exit on the left of the
sternum.
• One wire from each pair serves as a cathode
and an othere as a anode, allowing bipolar
sensing and pacing of either or both chambers.
6
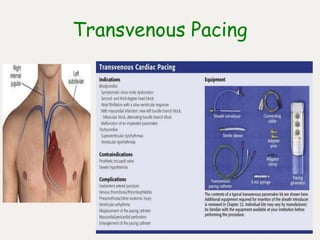
Transvenous Pacing
• Emergencyuse with external pacemaker
• Require central access and carries risk of
Bacteremia/infection.
• Appropriate placement should be guided by
fluoroscopy or echocardiography.
• Confirmation of position by plain film of
chest.
9
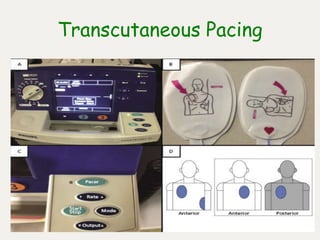
Transcutaneous Pacing
• Emergencyuse with external pacemaker
• Significant sedation is often required
due to the discomfort caused by this
method of pacing.
11
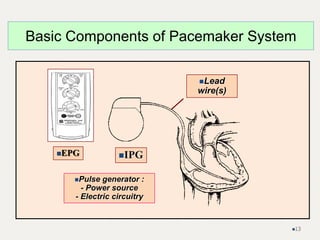
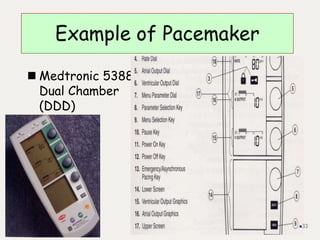
Pulse generator :
-Power source
- Electric circuitry
Lead
wire(s)
Basic Components of Pacemaker System
IPG
EPG
13
14.
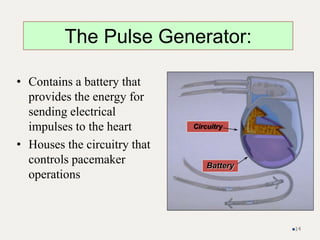
• Contains abattery that
provides the energy for
sending electrical
impulses to the heart
• Houses the circuitry that
controls pacemaker
operations
Circuitry
Battery
The Pulse Generator:
14
15.
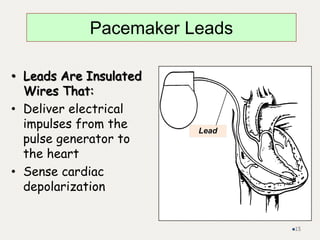
• Leads AreInsulated
Wires That:
• Deliver electrical
impulses from the
pulse generator to
the heart
• Sense cardiac
depolarization
Lead
Pacemaker Leads
15
16.
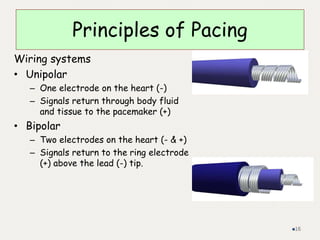
Principles of Pacing
Wiringsystems
• Unipolar
– One electrode on the heart (-)
– Signals return through body fluid
and tissue to the pacemaker (+)
• Bipolar
– Two electrodes on the heart (- & +)
– Signals return to the ring electrode
(+) above the lead (-) tip.
16
17.
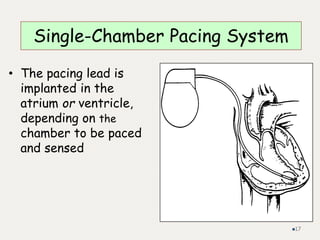
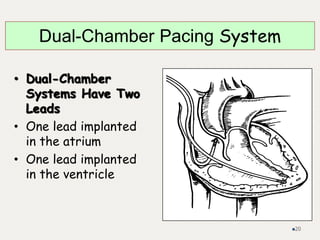
Single-Chamber Pacing System
•The pacing lead is
implanted in the
atrium or ventricle,
depending on the
chamber to be paced
and sensed
17
• Stimulate cardiacdepolarization
• Sense intrinsic cardiac function
• Respond to increased metabolic demand
by providing rate responsive pacing
• Provide diagnostic information stored by
the pacemaker
Most Pacemakers Perform Four Functions:
25
26.
Principles of Pacing
Modesof Pacing
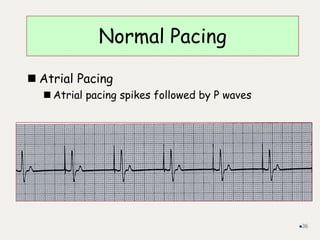
Atrial pacing
Intact AV conduction system required
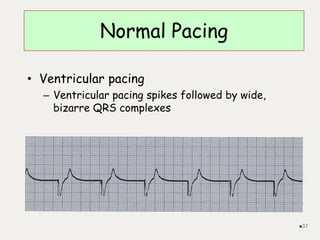
Ventricular pacing
Loss of atrial kick
Discordant ventricular contractions
Sustains cardiac output
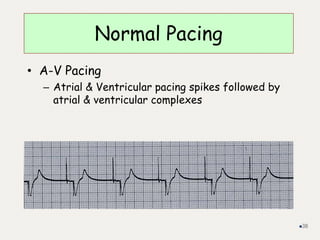
Atrial/Ventricular pacing
Natural pacing
Atrial-ventricular synchrony
26
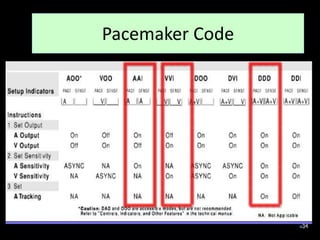
IN temporary pacemakeronly the first three
letters of the code are used.
The fourth letter in common use to denote
presence or absence of rate responsiveness in
permanent pacemaker.
The fifth letter of code in not commonly used
except in cardiac resynchronization therapy
(CRT) devices.
28
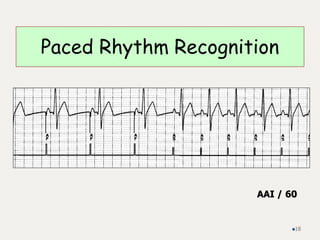
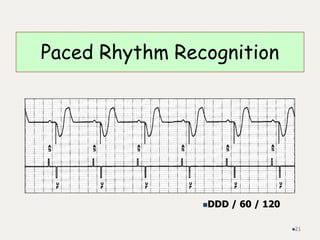
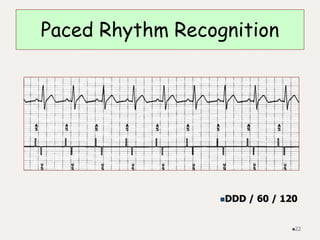
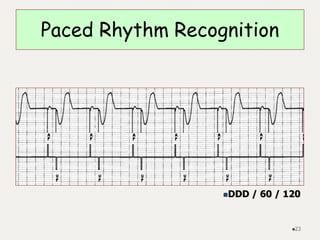
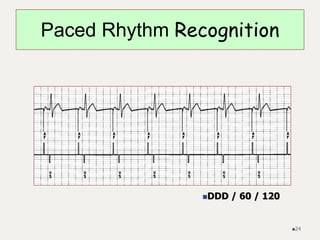
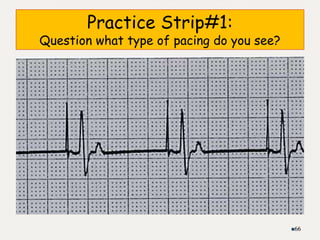
Pacemaker EKG Strips
•Assessing Paced EKG Strips
– Identify intrinsic rhythm and clinical condition
– Identify pacer spikes
– Identify activity following pacer spikes
– Failure to capture
– Failure to sense
• EVERY PACER SPIKE SHOULD HAVE A P-WAVE
OR QRS COMPLEX FOLLOWING IT.
35
Failure to capture:
•The pacemaker send
stimulus that is not
followed by
corresponding P or
QRS wave.
• You fixe it by adjusting
(Pacing) output and its
related connections
Failure to sense:
• The pacemaker did not
see the P or QRS wave
and send stimulus in
spite of that
• You fix it by adjusting
input (sensing
sensitivity) and its
related connections.
40
2 problem related to Pacemaker
functioning should be identified
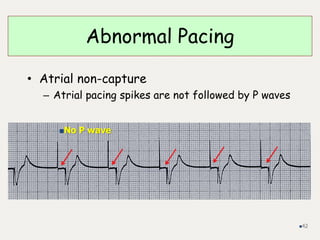
Abnormal Pacing
• Atrialnon-capture
– Atrial pacing spikes are not followed by P waves
42
No P wave
43.
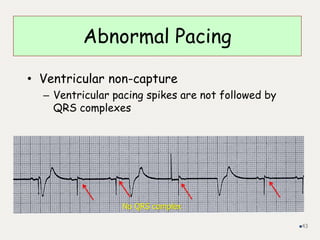
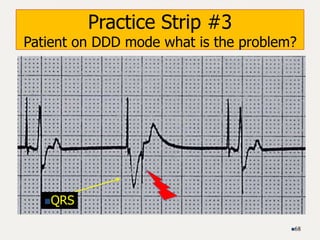
Abnormal Pacing
• Ventricularnon-capture
– Ventricular pacing spikes are not followed by
QRS complexes
43
No QRS complex
44.
Failure to Capture:
thepacing stimulus was not followed by P or
QRS wave (no chamber contraction)
• Causes
– Insufficient energy delivered by pacer
– Low pacemaker battery
– Dislodged, loose, fibrotic, or fractured electrode
– Electrolyte abnormalities
• Acidosis
• Hypoxemia
• Hypokalemia
• Danger - poor cardiac output
44
45.
• Solutions
– Viewrhythm in different leads
– Change electrodes
– Check connections
– Increase pacer output (↑mA)
– Change battery, cables, pacer
45
Failure to Capture
46.
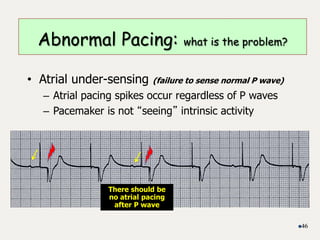
• Atrial under-sensing(failure to sense normal P wave)
– Atrial pacing spikes occur regardless of P waves
– Pacemaker is not “seeing” intrinsic activity
46
Abnormal Pacing: what is the problem?
There should be
no atrial pacing
after P wave
47.
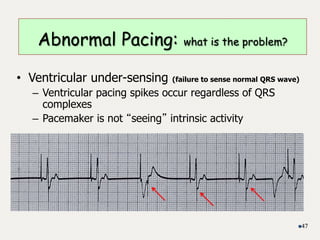
• Ventricular under-sensing(failure to sense normal QRS wave)
– Ventricular pacing spikes occur regardless of QRS
complexes
– Pacemaker is not “seeing” intrinsic activity
47
Abnormal Pacing: what is the problem?
48.
A basic principle
•The pacemaker works with this principle : If I see or receive (sense) stimulus (P/QRS) I
do not fire (Pace) , If I do not sense stimulus (P/QRS) I will fire (Pace). What makes the
pacemaker sees the intrinsic rhythm is pacemaker sensitivity (higher sensitivity
means less ability to see/hear intrinsic rhythm and that will result in more pacemaker
firing ). Less sensitivity means more ability to see intrinsic rhythm and less pacemaker
firing.
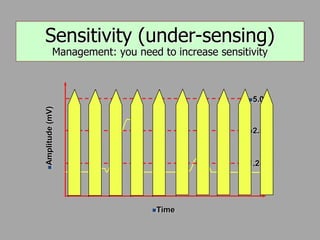
• Under-sensing means the pacemaker does not see intrinsic rhythm (P or QRS) so the
pacemaker will fire which will cause pacemaker impulse delivered in wrong time
(may lead to life threatening arrhythmia) or higher rate than needed due to frequent
pacing that is not needed
• The management of under-sensing by increasing pacemaker sensitivity (decrease
filtering so pacemaker sees and hears intrinsic rhythm) so the pacemaker does not
fire more than it should or fire during wrong timing.
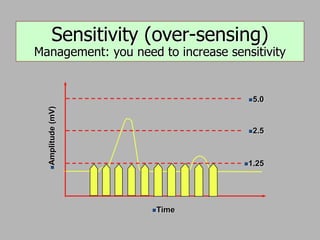
• Over sensing, the pacemaker sees too many artifacts and interpret them as normal P
or QRS leading to not delivering the impulse where it should be delivered (that will
result in slow inadequate rhythm or low cardiac output)
• The management of over-sensing is decrease sensitivity (increase filtering ability so
pacemaker sees and hears less surrounding artifacts) so pace maker fire more
appropriately.
48
49.
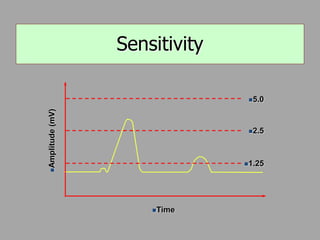
• Definition: Minimumlevel of intrinsic
electric activity generated by the heart
detectable by the pacemaker
4/07 49
Sensitivity Threshold
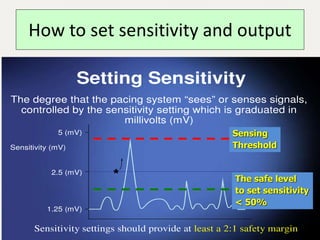
50.
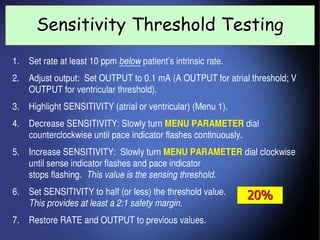
How to setsensitivity and output
50
Sensing
Threshold
The safe level
to set sensitivity
< 50%
51.
Sensitivity – TheGreater the Number, the Less
Sensitive the Device to Intra-cardiac Events
Failure to Sense:
Theheart own rhythm P or QRS /chamber
contraction was not recognized by pacemaker
• Causes
– Pacemaker not sensitive enough to patient’s
intrinsic electrical activity (mV)
– Insufficient myocardial voltage
– Dislodged, loose, fibrotic, or fractured
electrode
– Electrolyte abnormalities
– Low battery
– Malfunction of pacemaker or bridging cable
56
57.
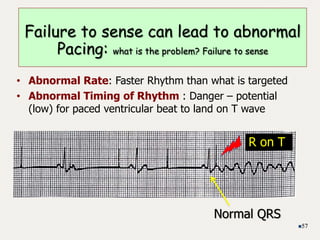
• Abnormal Rate:Faster Rhythm than what is targeted
• Abnormal Timing of Rhythm : Danger – potential
(low) for paced ventricular beat to land on T wave
57
Failure to sense can lead to abnormal
Pacing: what is the problem? Failure to sense
R on T
Normal QRS
58.
• Solution
– Viewrhythm in different leads
– Change electrodes
– Check connections
– Increase pacemaker’s sensitivity (↓mV)
– Change cables, battery, pacemaker
– Reverse polarity
– Check electrolytes
– Unipolar pacing with subcutaneous “ground wire”
58
Failure to sense
59.
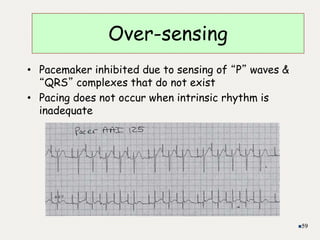
Over-sensing
• Pacemaker inhibiteddue to sensing of “P” waves &
“QRS” complexes that do not exist
• Pacing does not occur when intrinsic rhythm is
inadequate
59
60.
• Causes
– Pacemakerinhibited due to sensing of “P”
waves & “QRS” complexes that do not exist
– Pacemaker too sensitive
– Possible wire fracture, loose contact
– Pacemaker failure
• Danger - heart block, asystole
60
Over-sensing
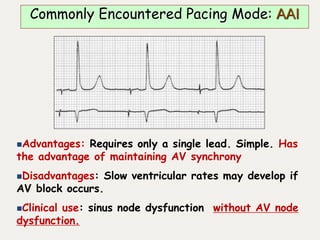
Advantages: Requires onlya single lead. Simple. Has
the advantage of maintaining AV synchrony
Disadvantages: Slow ventricular rates may develop if
AV block occurs.
Clinical use: sinus node dysfunction without AV node
dysfunction.
Commonly Encountered Pacing Mode: AAI
63.
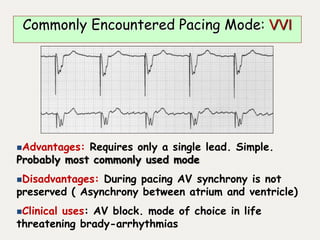
Advantages: Requires onlya single lead. Simple.
Probably most commonly used mode
Disadvantages: During pacing AV synchrony is not
preserved ( Asynchrony between atrium and ventricle)
Clinical uses: AV block. mode of choice in life
threatening brady-arrhythmias
Commonly Encountered Pacing Mode: VVI
64.
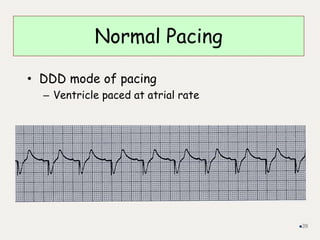
Advantages:AV synchrony ismaintained for
patients with sinus node and AV node disease
Disadvantages: Require two leads. More
complex
Clinical uses: Bradycardia caused by SND or
AV node disease
Commonly Encountered Pacing Mode: DDD
65.
Advantages: AV synchronyis maintained during
atrial pacing. Useful in patients with SA node
dysfunction and episodes of atrial tachyarrhythmias.
During atrial tachyarrhythmias pacemaker paces
ventricle at back-up rate and will not track
tachyarrhythmia
Disadvantages: AV synchrony is not maintained
during atrial sensing
Clinical uses: For patients with bradycardia and
intermittent atrial tachycardia
Commonly Encountered Pacing Mode: DDI
Answers
Mode of pacing,rhythm/problem, solution
1. AAI: normal atrial pacing
2. Sinus rhythm: no pacing; possible back-up setting AAI, VVI, DDD
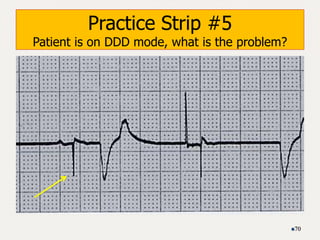
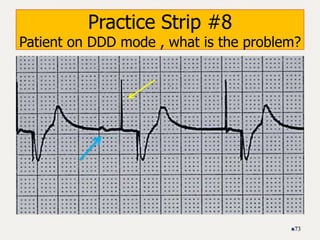
3. DDD: failure to sense ventricle; increase ventricular mA
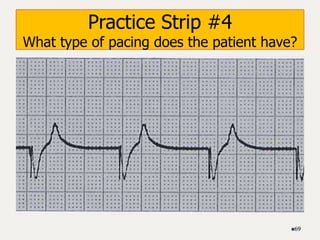
4. VVI: ventricular pacing
5. DDD: failure to capture atria or ventricle; increase atrial & ventricular
mA
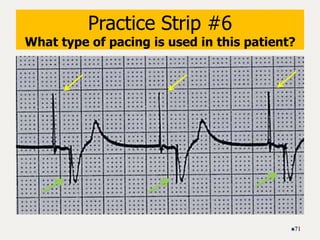
6. DDD: normal atrial & ventricular pacing
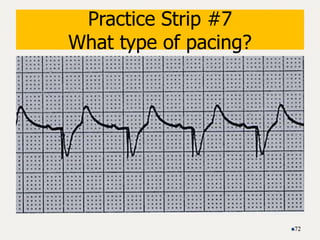
7. DDD: normal atrial sensing, ventricular pacing
8. DDD: failure to capture atria; increase atrial mA
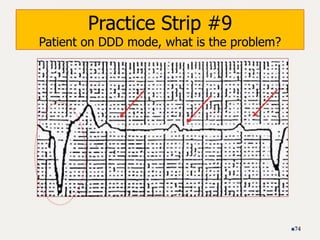
9. DDD: oversensing; decrease ventricular sensitivity
75
Editor's Notes
#57 The pacemaker works with this principle : If I see or receive stimulus (P/QRS) I do not fire , If I do not see stimulus (P/QRS) I will fire. What make the pacemaker sees the intrinsic rhythm is pacemaker sensitivity (higher sensitivity means more ability to see intrinsic rhythm and that will result in less pacemaker firing )
Under-sensing means the pacemaker does not see intrinsic rhythm (P or QRS) so the pacemaker will fire which will cause pacemaker impulse delivered in wrong time (may lead to life threatening arrhythmia) or higher rate than needed due to frequent pacing that is not needed
The management of under-sensing you increase pacemaker sensitivity (decrease filtering so pacemaker sees and hears intrinsic rhythm) so the pacemaker does not fire more than it should or fire during wrong timing.
Over sensing, the pacemaker sees too many artifacts and interpret them as normal P or QRS leading to not delivering the impulse where it should be delivered (that will result in slow inadequate rhythm or low cardiac output)
The management of over-sensing is decrease sensitivity (increase filtering ability so pacemaker sees and hears less surrounding artifacts) so pace maker fire more appropriately.
If you want more beats from pacemaker decrease sensitivity
If you want less beats from pacemaker increase sensitivity
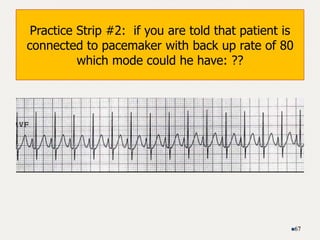
#65 Inhibited Pacing of the Atrium and Ventricle (DDI)In the DDI pacing mode, there is sensing in both the atrium and the ventricle, but the only response to asensed event is inhibition (Fig. 1). If the pacemaker senses atrial activity, it does not deliver an atrial stimulus,and the timer of the atrioventricular interval does not start, so that the pacemaker neither delivers ventricularoutput in response to spontaneous atrial activity nor “tracks” such activity. The atrioventricular-interval timer starts only after a paced atrial event; atrioventricularsynchrony is present only while the atrium is being paced or during sinus rhythm, provided that the patient has intact atrioventricular-node conduction. In DDI pacing, the paced rate is never higher than the pro-grammable low rate interval; no adaptation of the rate occurs unless the sinus node responds appropriately to increased metabolic demand (a response defined as “chronotropic competence”) and the patient has intact atrioventricular-node conduction. DDI pacing (particularly the DDIR mode) may be suitable when there are frequent atrial tachyarrhythmias that might be inappropriately tracked by a DDD pacemaker, resulting in rapid paced ventricular rates.
36
#76 AAI: normal atrial pacing
Sinus rhythm: no pacing; possible back-up setting AAI, VVI, DDD
DDD: failure to sense ventricle; increase ventricular mA
VVI: ventricular pacing
DDD: failure to capture atria or ventricle; increase atrial & ventricular mA
DDD: normal atrial & ventricular pacing
DDD: normal atrial sensing, ventricular pacing
DDD: failure to capture atria; increase atrial mA
DDD: oversensing; decrease ventricular sensitivity