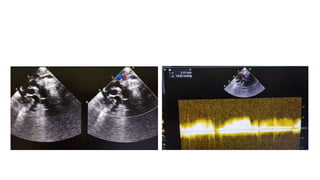
1) A 24-day-old neonate presented with cyanosis since birth and difficulty breathing. Echocardiography showed supracardiac total anomalous pulmonary venous return with vertical vein obstruction.
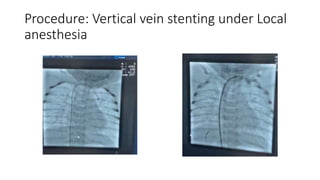
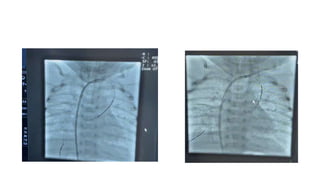
2) The baby underwent vertical vein stenting under local anesthesia to treat the obstruction.
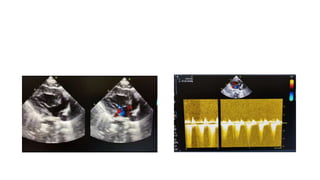
3) Follow-up echocardiography after the procedure showed improvement, with stents in the vertical vein and only mild tricuspid regurgitation. The procedure successfully treated the vertical vein obstruction.

























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





