2
Hematopoietic Malignancies
Lymphoma isa general term used for proliferations that
arise as discrete tissue masses.
Leukemia is used for neoplasms that present with
widespread involvement of the bone marrow and the
peripheral blood(usually).
3.
3
What is Lymphoma
Malignantlymphoma is a term given to tumors of the
lymphoid system and specifically of lymphocytes and
their precursor cells
i.e.
Cancer of the lymphatic system.
• Many lymphomas are known to be due to specific
genetic mutations.
5
Hodgkin disease
Hodgkin lymphoma
Typeof malignant lymphoma in which Reed-Sternberg cells are present in
a characterstic background of reactive inflammatory cells of various types,
accompanied by fibrosis of variable degree.
( except NLPHL)
7
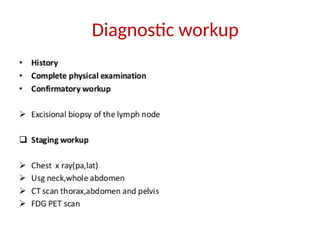
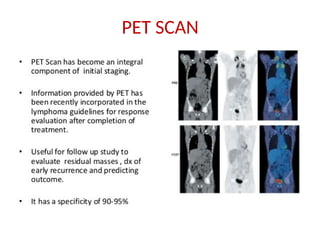
Introduction
• Are groupof cancers which originate from lymphatic systems.
• It was named after Thomas Hodgkin who first described it in 1832.
• Dorothy Reed and Carl Sternberg first described the malignant cells of
Hodgkin lymphoma call Reed Sternberg cells.
• Hodgkin lymphoma was the first cancer which could be successfully
treated by radiation therapy and also by combination chemotherapy.
9
Risk Factors
• Noclear risk factors, several implicated
• EBV (pathogen or passenger)
• HIV
• woodworking, farming
• rare familial aggregations
• First degree relatives have five fold increase in risk for Hodgkin lymphoma.
• Associated with EBV infection mainly with mixed cellularity type.
• High socio economic status.
• Prolonged use of of human growth hormone.
• men > women
• whites > blacks > Asians
10.
10
Natural history
• Hodgkinlymphoma arises in a single node or chain of nodes and spreads
first to anatomically contiguous lymphoid tissue.
• Visceral involvement by hodgkin lymphoma may be secondary to
extension from adjacent lymph nodes.
• Hematogenous spread occurs to liver or multiple bony sites.
• Mechanism of spleen involvement is unclear but all patients with hepatic
and bone involvement are associated with splenic involvement.
11.
11
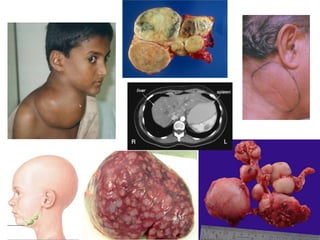
Clinical features
• Mostcommon presentation is asymptomatic lymphnode enlargement,
typically in the neck.
• Cervical lymphnodes are involved in 80% cases.
• Mediastinal involvement is seen in about 50% cases. They produce
symptoms like chest pain, cough and dyspnoea.
• Infradiaphrgamatic involvement is seen in 5% cases and usually seen with
older patients.
• Other less common symptoms are :
Pruritis, alcohol induced pain over involved lymphnodes, nephrotic syndrome,
erythema nodosum, cerebellar degeneration, immune hemolytic
anaemia, thrombocytopenia, hypercalcemia.
12.
12
B symptoms
• About33 % present with B symptoms overall
• Only 15-20% of stage I-III have B symptoms like
1. Fever(>38^C)
• May first present as fever of unknown origin
• Fever persists for days to weeks followed by afebrile intervals and then
recurrence.
• This pattern is called Pel Ebstein fever.
2. Drenching night sweats
3. Weight loss (>10% in 6 months)
18
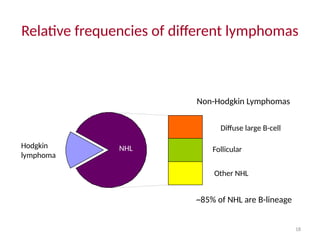
Relative frequencies ofdifferent lymphomas
Hodgkin
lymphoma
NHL
Diffuse large B-cell
Follicular
Other NHL
Non-Hodgkin Lymphomas
~85% of NHL are B-lineage
19.
19
Hodgkin lymphoma
• Cellof origin: Germinal centre B-cell
• Reed-Sternberg cells (or RS variants) in the affected
tissues.
• Most cells in affected lymph node are polyclonal
reactive lymphoid cells, not neoplastic cells.
20.
20
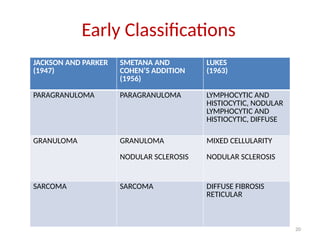
JACKSON AND PARKER
(1947)
SMETANAAND
COHEN’S ADDITION
(1956)
LUKES
(1963)
PARAGRANULOMA PARAGRANULOMA LYMPHOCYTIC AND
HISTIOCYTIC, NODULAR
LYMPHOCYTIC AND
HISTIOCYTIC, DIFFUSE
GRANULOMA GRANULOMA
NODULAR SCLEROSIS
MIXED CELLULARITY
NODULAR SCLEROSIS
SARCOMA SARCOMA DIFFUSE FIBROSIS
RETICULAR
Early Classifications
21.
21
Later Classifications
• TheLukes-Butler classification of HL, modified at the Rye Conference in
1966, described the criteria for the four familiar subtypes of HL:
lymphocyte-predominant, nodular sclerosing, mixed cellularity, and
lymphocyte-depleted.
• The REAL classification separated the nodular lymphocyte-predominant
(NLP) subtype from so-called classic HL based on the immunophenotypic
and genotypic differences
• The REAL classification of HL was carried forward to the 2001 WHO
classification of HL and the 2008 WHO classification.
23
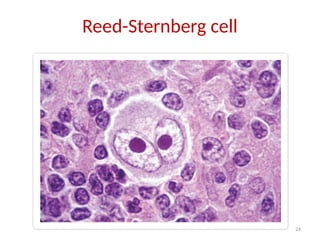
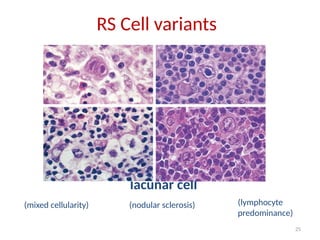
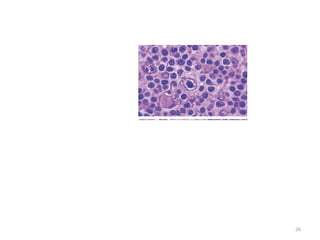
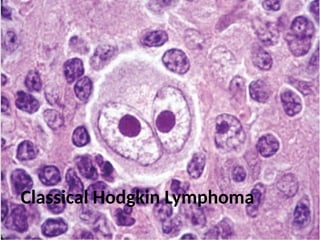
Reed Sternberg cell
Commonfeature of ALL Hodgkin Lymphomas.
• Large cells ( >45um in diameter) with classically binucleate or bilobed
central nucleus each with a large acidophilic central nucleoli surrounded
by a clear halo. “owl’s eye appearance”
• Variants: mononuclear (Hodgkin’s cell), mummified cell, lacunar cell, L/H
cell.
• Requirement of Reed-Sternberg cell for initial diagnosis is “absolute”(less
strict for LPHL or recurrent disease)
• Classic Reed-Sternberg cell:
+ CD15, CD30, CD25
– CD45, pan-B, S-100, keratin, EMA
• Most current studies indicate the RS cells of HL are lymphocytic in nature
and, in the great majority of cases, are of B-cell origin.
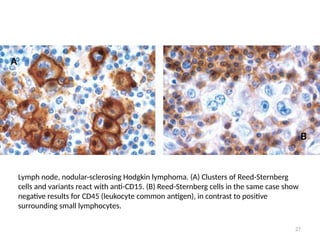
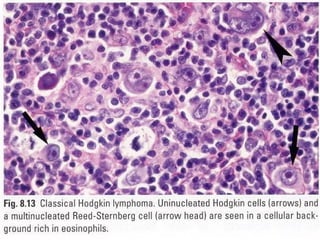
27
Lymph node, nodular-sclerosingHodgkin lymphoma. (A) Clusters of Reed-Sternberg
cells and variants react with anti-CD15. (B) Reed-Sternberg cells in the same case show
negative results for CD45 (leukocyte common antigen), in contrast to positive
surrounding small lymphocytes.
A
B
28.
28
A possible modelof pathogenesis
germinal
centre
B cell
transforming
event(s)
loss of apoptosis
RS cell
inflammatory
response
EBV?
cytokines
29.
29
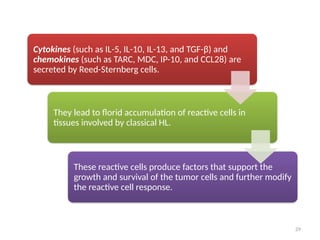
Cytokines (such asIL-5, IL-10, IL-13, and TGF-β) and
chemokines (such as TARC, MDC, IP-10, and CCL28) are
secreted by Reed-Sternberg cells.
They lead to florid accumulation of reactive cells in
tissues involved by classical HL.
These reactive cells produce factors that support the
growth and survival of the tumor cells and further modify
the reactive cell response.
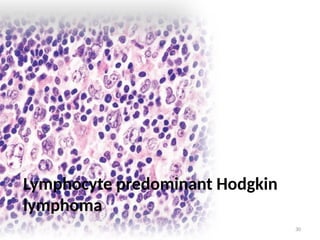
31
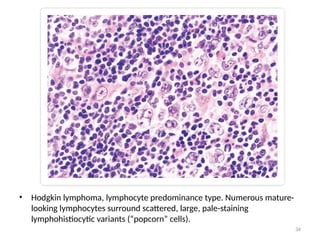
Lymphocyte predominant Hodgkin
lymphoma
•<5% of Hodgkin lymphoma
• Mainly involves cervical, axillary or mediastinal
• L&H cells or Popcorn cells are seen
• Positive for CD20, 45, CD79a, Bcl-6, J-chain, and PAX-5. EMA positive
in 50% cases.
• Negative for CD15, 30.
• Differential Diagnosis: Well differentiated lymphocytic lymphoma,
mononucleosis, malignant melanoma,, progressive transformation of
germinal centers
32.
32
• LPHL isdivided into two histopathologic subtypes:
1. Lymphocytic and histiocytic (L&H) nodular
2. L&H diffuse
• Currently the WHO classification recognizes only the nodular type and
requires at least a partially nodular growth pattern for diagnosis . Whether
the diffuse type is a distinct entity is controversial.
• Small lymphocytes predominate in the reactive component in both types
and are intermixed with varying numbers of histiocytes. Eosinophils,
neutrophils, and “diagnostic” or “classic” RS cells are rare. In fact, the
diagnosis of LPHL is doubtful if diagnostic RS cells are found easily; the
number of such cells should be fewer than one per histologic section.
33.
33
• In LPHL,L&H variants of RS cells are conspicuous with folded, multilobed
nucleus and smaller nucleoli(“popcorn nuclei”).
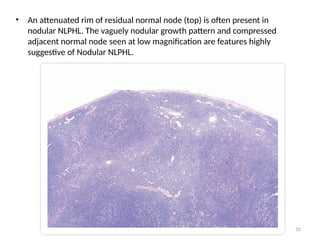
• In the nodular subtype of LPHL, there is almost total obliteration of the
nodal architecture by a vaguely nodular process. LPHL nodules are
composed of small, round lymphocytes with varying numbers of
epithelioid histiocytes which gives them a mottled appearance. L&H
variants of RS cells may be numerous and are principally seen in the
nodules.
• “Diagnostic” or “classic” RS cells are rare or nonexistent and are not
required for the diagnosis of NLPHL.
35
• An attenuatedrim of residual normal node (top) is often present in
nodular NLPHL. The vaguely nodular growth pattern and compressed
adjacent normal node seen at low magnification are features highly
suggestive of Nodular NLPHL.
37
1. Nodular Sclerosis
•Most common type diagnosed
• About 70%
• Lacunar cells seen
• CD15, 30 positive
• EBV negative
• Only subtype without a male predominance
• Seen in younger patients with stage I-II disease.
• Differential diagnosis: Large cell Non Hodgkin lymphoma, carcinoma,
germ cell tumour and thymoma.
38.
38
The classic histopathologiccriteria for NSHL are
(a) prominent nodularity
(b) presence of lacunar RS cell variants, and
(c) birefringent broad collagen bands
• Nodal architecture is obliterated by relatively large nodules of tumor
partly or totally encircled by dense connective tissue bands that are
birefringent when viewed under polarized light.
39.
39
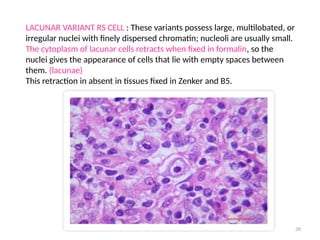
LACUNAR VARIANT RSCELL : These variants possess large, multilobated, or
irregular nuclei with finely dispersed chromatin; nucleoli are usually small.
The cytoplasm of lacunar cells retracts when fixed in formalin, so the
nuclei gives the appearance of cells that lie with empty spaces between
them. (lacunae)
This retraction in absent in tissues fixed in Zenker and B5.
40.
40
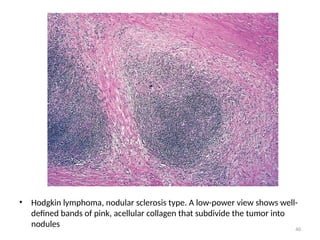
• Hodgkin lymphoma,nodular sclerosis type. A low-power view shows well-
defined bands of pink, acellular collagen that subdivide the tumor into
nodules
41.
41
2. Mixed Cellularity
•Constitutes about 20%
• More than 50% present as stage III or IV disease
• Biphasic incidence, peaking in young adults and again in adults
older than 55
• CD15, 30, EBV positive
• Presents in advanced stages
• Tendency to involve spleen, bone marrow.
• Differential diagnosis: Some cases of MCHL display an interfollicular
growth pattern. Such cases may be difficult to distinguish from peripheral
T-cell lymphomas. Lennert’s lymphoma (diffuse mixed T-cell ML with
excessive histiocytes). Diffuse follicular lymphoma.
42.
42
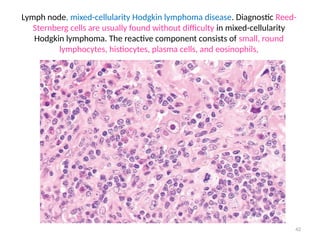
Lymph node, mixed-cellularityHodgkin lymphoma disease. Diagnostic Reed-
Sternberg cells are usually found without difficulty in mixed-cellularity
Hodgkin lymphoma. The reactive component consists of small, round
lymphocytes, histiocytes, plasma cells, and eosinophils,
43.
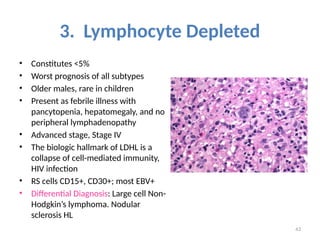
43
3. Lymphocyte Depleted
•Constitutes <5%
• Worst prognosis of all subtypes
• Older males, rare in children
• Present as febrile illness with
pancytopenia, hepatomegaly, and no
peripheral lymphadenopathy
• Advanced stage, Stage IV
• The biologic hallmark of LDHL is a
collapse of cell-mediated immunity,
HIV infection
• RS cells CD15+, CD30+; most EBV+
• Differential Diagnosis: Large cell Non-
Hodgkin’s lymphoma. Nodular
sclerosis HL
44.
44
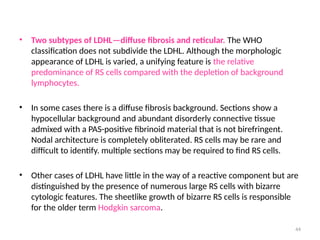
• Two subtypesof LDHL—diffuse fibrosis and reticular. The WHO
classification does not subdivide the LDHL. Although the morphologic
appearance of LDHL is varied, a unifying feature is the relative
predominance of RS cells compared with the depletion of background
lymphocytes.
• In some cases there is a diffuse fibrosis background. Sections show a
hypocellular background and abundant disorderly connective tissue
admixed with a PAS-positive fibrinoid material that is not birefringent.
Nodal architecture is completely obliterated. RS cells may be rare and
difficult to identify. multiple sections may be required to find RS cells.
• Other cases of LDHL have little in the way of a reactive component but are
distinguished by the presence of numerous large RS cells with bizarre
cytologic features. The sheetlike growth of bizarre RS cells is responsible
for the older term Hodgkin sarcoma.
45.
45
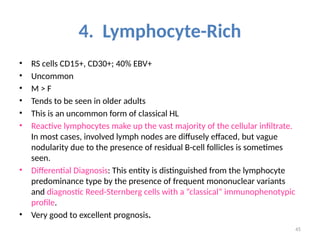
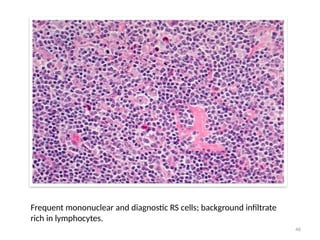
4. Lymphocyte-Rich
• RScells CD15+, CD30+; 40% EBV+
• Uncommon
• M > F
• Tends to be seen in older adults
• This is an uncommon form of classical HL
• Reactive lymphocytes make up the vast majority of the cellular infiltrate.
In most cases, involved lymph nodes are diffusely effaced, but vague
nodularity due to the presence of residual B-cell follicles is sometimes
seen.
• Differential Diagnosis: This entity is distinguished from the lymphocyte
predominance type by the presence of frequent mononuclear variants
and diagnostic Reed-Sternberg cells with a “classical” immunophenotypic
profile.
• Very good to excellent prognosis.
48
Spread
• Generally awell behaved spread of disease through contiguous LN groups,
(especially NS and LP); <5% show non-contiguous spread
• May have direct extension into perinodal tissue.
• 85% of Stage I/II disease are above diaphragm.
• Spleen: if >400g, almost always positive.
• Liver: if positive, spleen and retroperitoneal LN’s are also positive.
49.
49
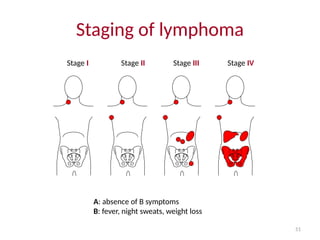
Ann Arbor StagingSystem
• Stage I: Single lymph node region (I) or single extralymphatic organ or
site (IE)
• Stage II: > 2 lymph node regions on same side of diaphragm (II) or with
limited, contiguous extra lymphatic tissue involvement (IIE)
• Stage III: both sides of diaphragm involved, may include spleen (IIIS) or
local tissue involvement (IIIE)
• Stage IV: multiple/disseminated foci involved with > 1 extralymphatic
organs (i.e. bone marrow)
(A) or (B) designates absence/presence of “B” symptoms
*(E) Localized, solitary involvement of extralymphatic tissue, excluding liver
and bone marrow
51
Stage I StageII Stage III Stage IV
Staging of lymphoma
A: absence of B symptoms
B: fever, night sweats, weight loss
52.
52
PROGNOSIS
• Clinical stage
•Extranodal involvement bad (especially if distant rather than by direct
spread)
• Degree of splenic involvement: ≥5 nodules poor prognosis
• Age: >50 yrs unfavorable
• Sex and race: Black males worse than white females
• Microscopic type: LP and NS best, MC intermediate, LD worst (less
important with current treatment protocols)
• Laboratory findings: decreased hematocrit, elevated LDH, raised ESR,
elevated serum levels of CD30, soluble CD25 have negative prognosis.
• CD15- lack of expression is a negative prognostic factor.
55
Radiotherapy
• Radiation therapyis the most effective single thrapeutic agent for treating
Hodgkin lymphoma.
• The main objective of radiation in Hodgkin lymphoma is to treat involved
and contiguous field.
• Radiotherapy can be given by
1. 2D planning
2. 3D planning
3. IFRT
• Involved field radiotherapy is the most commonly used technique at
present. It targets a smaller area rather than a classical extended field.
56.
56
Complications
• Autologous bonemarrow transplantation can cure half of patients who fail
effective chemotherapy regimens.
• Because of the very high cure rate in patients with Hodgkin's disease,
long-term complications have become a major focus for clinical research.
The most serious late side effects include secondary malignancies, cardiac
injury, infertility and Lhermitte's syndrome.