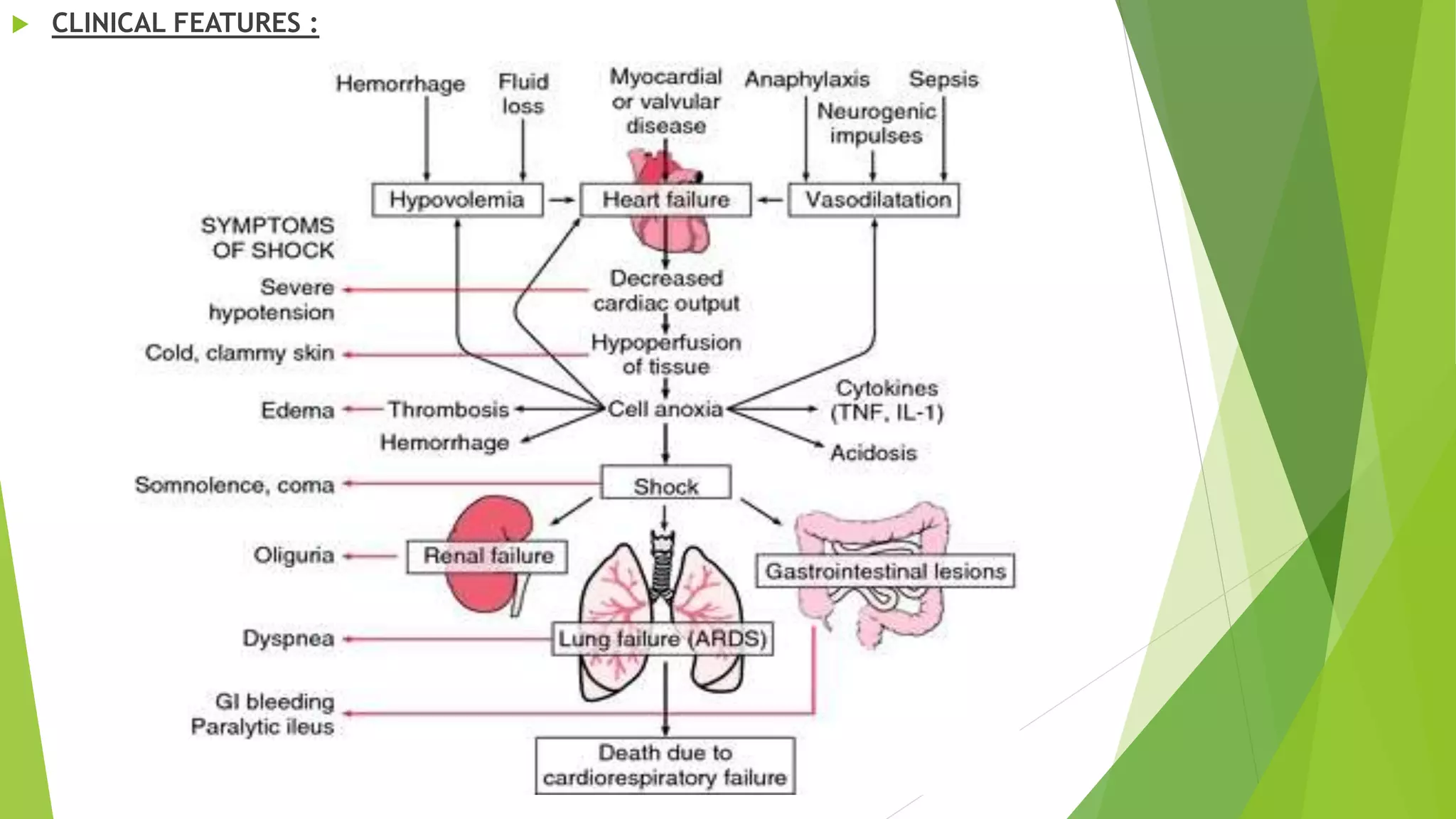
The document discusses the systemic effects that can result from injury, including immediate effects like hypovolemic shock from blood loss, as well as early effects like acute respiratory distress syndrome, fat embolism, deep vein thrombosis, pulmonary embolism, traumatic fever, and crush syndrome. Later systemic effects include sepsis. Specific conditions like hypovolemic shock, acute respiratory distress syndrome, fat embolism syndrome, and crush syndrome are then described in more detail, outlining their causes, clinical features, diagnostic findings, and management.