Chief Complaints
Painabdomen
Vomiting
Sensation of fullness after meals
Vomiting of blood
Passage of black tarry stool
Yellowish discoloration of eyes and
urine
Loss of appetite
Weight loss
Alteration of bowel habit
Detailed history aboutpain
− Onset: Sudden/insidious
− Duration: Short-lived/persistent
− Initial site of pain
− Radiation/Shifting/Referral
−Character of pain: Dull-aching (chronic
cholecystitis)/stabbing
(pancreatitis)/colicky (renal colic).
−Periodicity of pain: Appearance after a
definite period of days/months
8.
− Relation withfood intake: Before/after,
i.e. on empty stomach or full stomach
− Relation with vomiting:
Relief/aggravation
−Aggravating and relieving factors:
Food/vomiting/medicines
− Relation with defecation and
micturition
11.
Details of vomiting
−Duration
− Frequency: exact number
− Relationship with food intake
− Character of the act: Projectile or
effortless
− Character of the vomitus
− Amount
− Color
− Taste
− Smell
12.
−Contains any foodtaken more than 12
hours earlier
−Any blood in vomiting: Suggestive of
upper gastrointestinal bleeding
− Any relation with pain
13.
Details of bloodvomiting
(Hematemesis)
− Duration
− Number of bouts of blood vomiting
− Color
− Amount
− Whether associated with black tarry
stool or not
14.
Details of jaundice
−Duration
− Onset
− Any prodromal symptom before onset
of jaundice: Fever/arthralgia/generalized
weakness/loss of appetite/skin rash
suggestive of viral-hepatitis
− Any history of biliary colic preceding the
onset of jaundice
− Progress of jaundice
15.
− Progressively increasing
−Diminishing after an initial deepening
− Waxing and waning
− Static
−Associated symptoms with jaundice:
» Pruritis: obstructive jaundice
» Clay colored stool: Obstructive jaundice
− History of fever with chill and rigor—
cholangitis
16.
− History ofbiliary colic
− History of black tarry stool with waxing
and waning of jaundice.
17.
Bowel habit
− Whatwas the usual bowel habit before
the illness started?
− What is the present bowel habit?
− What is the change in bowel habit?
− Any history of bleeding P/R or black
tarry stool, passage of mucus in stool
− Any history of sensation of incomplete
defecation
− Any history of tenesmus
18.
Other
Details ofloss of weight and appetite:
„
To mention exact figure of weight loss
in kilogram and the duration.
Details of swelling in the abdomen
Duration
Site where first noticed
Size of of the swelling when first
noticed
Progress of the swelling
19.
Details ofurinary symptoms:
Loin pain/mass in loin/frequency of
micturition (diurnal and
nocturnal)/difficulty in passing
urine/any burning during
micturition/any urgency or
hesitancy/any history of passage of
blood or pus in urine.
Inspection
Patient supinewith arms kept on sides
and exposed from mid-chest to mid-
thigh
−Shape and contour of abdomen »
Normal/Scaphoid/Distended
−Umbilicus » Position (normal position
lies midway between the xiphisternum
and the symphysis pubis) » Normally
inverted/deeply
inverted/flushed/everted.
31.
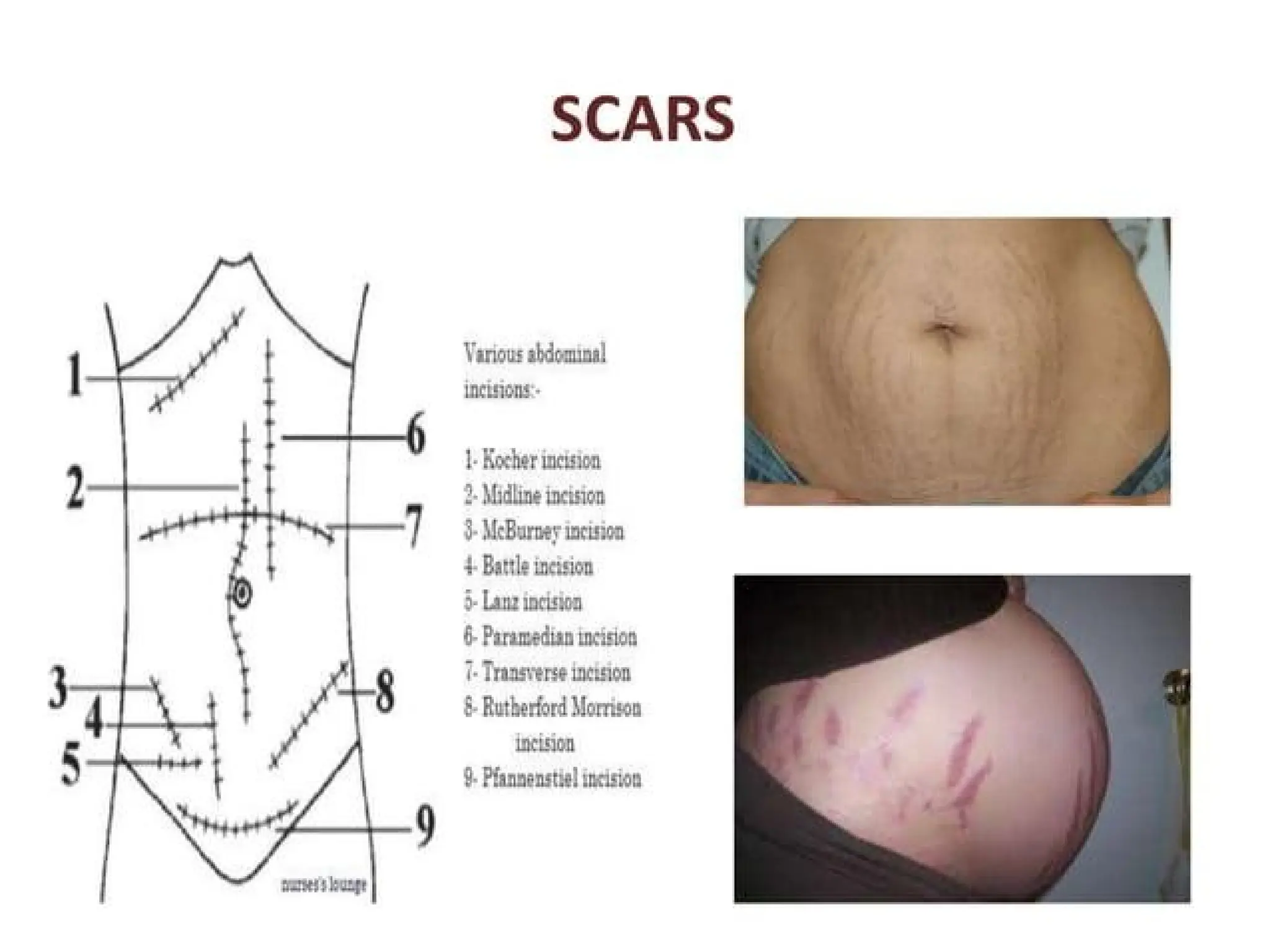
− Skin overthe abdomen
» Scar (If operative scar describe as upper
midline/lower midline/upper paramedian/
right or left subcostal incision scar)
» Pigmentation
» Striae (white striae found in multiparous
women is to be described as striae albicans)
» Engorged vein (if engorged veins are
present ascertain the direction of blood flow
in the engorged veins)
32.
− Movements
»Respiratory movementswhether all
region are moving normally with
respiration
» Visible peristalsis
» Pulsatile movements
− Visible swelling
» Site and extent
» Size
33.
» Shape
» Surface
»Margin
» Moving with respiration or not
» Rising test—whether swelling is parietal or
intra-abdominal
- Hernial sites
» Any swelling
» Any expansile impulse on cough
Palpation
Superficial palpation:
»Temperature: Examine all the regions of the
abdomen (Compare temperature of
abdomen with temperature of chest with
the dorsum of finger)
» Any superficial tenderness
» Feel of the abdomen: - Soft and elastic feel
is normal - Muscle guard - Rigidity
» Lump palpable: Details of the lump are to
be described under deep palpation
51.
Deep palpation:
Gastric point: A point in the midepigastrium.
Duodenal point: A point in the transpyloric
plane 2. 5 cm to the right of midline.
Gallbladder point: A point at the junction of
lateral border of right rectus abdominis and
the tip of right 9th costal cartilage.
McBurney’s point: A point in the right
spinoumbilical line at the junction of medial
two-thirds and lateral one-third.
52.
Amebic point:Point on left
spinoumbilical line corresponding to
McBurney’s point on right side.
Renal point: A point at the junction of
lateral border of erector spinae and
the 12th rib
54.
Palpation of lump
−Position and extent in relation to
abdominal regions
− Shape
− Size
− Surface
− Margin
− Consistency
− Mobility: with respiration
− Mobility from side to side, up and
down
55.
− Fixity toskin or underlying structure
− Rising test to confirrm intra-abdominal
or parietal swelling
− Knee elbow position and examine the
swelling again to decide whether
swelling is intraperitoneal or
retroperitoneal
81.
Percussion
− Normal percussionnote over the
abdomen
− Shifting dullness
− Fluid thrill
− Succusion splash over stomach
− Upper border of liver dullness
− Upper border of splenic dullness
− Percussion over any abdominal lump
palpable
Peristaltic movements inthe
abdomen
Gross peristaltic waves may be seen on
simple inspection.
Sit by the side of the patient and look
tangentially. Ask the patient to take a
deep breath and hold the breath at the
end of expiration so long he can.
Observe for any visible peristaltic wave.
If peristaltic waves are seen describe
the character of the peristaltic wave .
99.
Gastric peristalticwaves are large peristaltic
waves seen in epigastrium, umbilical or as
low as hypogastrium moving from left to
right.
Small intestinal peristaltic waves are seen in
central abdomen showing in step ladder
pattern.
Peristaltic waves in transverse colon may be
seen in right hypochondrium, epigastrium,
umbilical and left hypochondrium,
Pulsation in abdomen
Patient lies supine. Examiner looks
tangentially from the side to look for any
pulsation in the abdomen. Patient is asked
to hold the breath at the end of expiration to
obscure the respiratory movement so that
pulsation, if present, is seen well.
This is done by palpation. The index and the
middle fingers of both hands are placed
close to each other on the epigastrium on
either side of the midline.
102.
In caseof transmitted pulsation all the
fingers are simply lifted up.
In case of expansile pulsation the
fingers of two hands are lifted up and
are also separated.
103.
Palpation of theabdomen
Palpation is done with the patient supine,
with the arms by the side of the patient and
asking the patient to take deep breathing
with the mouth open.
The abdominal muscle gets relaxed during
expiration and in the pause between
inspiration and expiration.
The forearm of the clinician should be kept
horizontally at the same level of the
abdomen.
104.
Palpate witha warm hand particularly
during winter.
If hands are cooler rub two hands
together to make the hand warm
before palpating the abdomen.
The palpation is best done with the
flexor surfaces of the fingers and not
with the tip of the fingers.
105.
Temperature of abdomen
It is done by palpating with the back of
the fingers in all the quadrants of the
abdomen.
The temperature of the abdomen is
compared with the temperature of the
chest or the other covered parts of the
body.
106.
Engorged veins inthe abdominal
wall
In normal persons the flow in the veins
in abdominal wall is away from the
umbilicus both above and below the
umbilicus.
Engorged veins in the abdominal wall
may be due to: „
Portal hypertension „
Inferior vena cava obstruction „
Superior vena cava obstruction
107.
The directionof flow may be ascertained by
palpation.
Empty a segment of vein above the umbilicus
by milking with index finger of both hands.
Remove the lower finger: If the vein remains
collapsed, the flow is from above downward.
The veins fill quickly, if the flow is from below
upward.
Empty the vein segment in the same way.
108.
Remove theupper finnger: The vein remains
collapsed if the flow is from below upward.
The vein fills quickly, if the flow is from above
downward.
The same procedure is repeated by emptying
a segment of vein below the umbilicus.
In portal hypertension the flow will be away
from the umbilicus in both segments of the
vein below and above the umbilicus.
109.
In inferiorvena cava obstruction, the
flow will be from below to up in both
segments of the vein.
In superior vena cava obstruction, the
flow will be from above to down in both
segments of the vein.
110.
Feel of theabdomen
The feel of the abdomen is assessed
during superficial palpation.
The normal feel of the abdomen is soft
and elastic.
As the abdomen is pressed it yields and
on release the abdomen recoils back to
original position.
In perforative peritonitis there may be
muscle guard or rigidity.
111.
In presenceof muscle guard, there is
resistance when trying to yield the
abdomen.
In case of rigidity the abdomen cannot
be yielded at all.
This can be better appreciated by
palpating with two hands one placed
over the other.
The lower hand is pressed by the upper
hand gently and the feel of the
112.
Palpate liver
Patientsupine with legs flexed at the
hips and knees.
Place the hand flat on the abdomen
parallel to the right costal margin with
the fingers pointing upward and placed
lateral to the rectus muscle and the
fingertips are placed to lie parallel to
the edge of the liver.
Start palpating from the right iliac fossa
and move upward.
113.
Ask thepatient to take deep breaths with
open mouth.
With each expiration the hand is moved
nearer to the right costal margin.
If the liver is enlarged the margin of the
liver will ride over the tip of the fingers.
Palpate the margin of the liver—sharp,
rounded, firm, smooth or irregular.
Using the palmar aspect of the fingertips
the
114.
margin and thesurface of the liver is palpated
by changing the position of the fingertips
along the surface and margin of the liver.
Alternatively the enlarged liver border may be
palpated with the radial border of the index
finger.
Start palpating from right iliac fossa toward
the right costal margin keeping the radial
border of index finger parallel to the right
costal margin.
115.
Describe theenlargement as . . . cm. below
the right costal margin.
Start percussing in the right midclavicular
line at 2nd intercostal space, and if, clear
resonant note is obtained percuss
downward until a dull note is obtained. This
marks the upper border of liver dullness.
In infants below 3 years of age liver may be
palpable 2–3 fingers breadth below the
right
116.
costal margin.
Inhealthy thin adult liver may be
palpable just below the costal margin.
Palpation of liver in presence of ascites
is done by dipping method. The pulp of
the fingers is placed on the abdominal
wall. By a quick push the fingers are
dipped into the abdominal wall. The
enlarged liver may be felt by the
dipping fingers.
117.
Palpate the gallbladder
The normal gallbladder is not palpable.
The method for palpation of
gallbladder is same as for liver.
If the gallbladder is enlarged, it is
palpated in the right lumbar or even in
right iliac fossa.
Its lower margin, lateral and medial
margins are palpable and the upper
margin either becomes continuous with
the enlarged liver or passes under the
118.
Murphy’s sign
InMoynihan’s method for elicitation of
Murphy’s sign, the patient lies supine.
Place the left hand on the right costal
margin so that the thumb lies over the
region of the fundus of gallbladder (area
just lateral to the junction of the lateral
border of right rectus abdominis and the tip
of the right 9th costal cartilage).
Exert moderate pressure with the thumb
and ask the patient to take deep breaths.
119.
At theheight of inspiration when the inflamed
gallbladder impinges on the thumb there will
be a catch in breath and patient will wince with
pain. The Murphy’s sign is said to be positive.
This sign may also be elicited with the patient
in sitting position keeping hand in the right
costal margin as described above. This is found
in acute cholecystitis. Not found in chronic
cholecystitis or uncomplicated gallstone
disease.
120.
Palpate the spleen
The normal spleen is not palpable and
becomes palpable only when enlarged 1. 5
or 2 times the normal.
The spleen enlarges toward the right iliac
fossa after emerging from below the left
costal margin.
Patient supine with the arms by the side of
the patient: the left hand is placed over the
left lateral chest wall exerting some
amount of compression.
121.
Start palpatingfrom the right iliac fossa with the
fingertips pointing toward the left costal margin.
Ask the patient to take deep breathing.
At the zenith of inspiration, if the spleen is
enlarged the edge of the spleen will ride over
the tip of the fingers.
Spleen may also be palpated with the radial
border of the index finger starting from the
right iliac fossa and moving upwards towards
the left costal margin.
122.
Palpation byhooking for minor
enlargement: Patient supine with the
arms by the side of the patient and
knees flexed.
Patient’s left fist is placed behind the
left side of chest pushing forward.
The clinician stands on the left side of
the patient and places the fingers of the
hand below the left costal margin.
123.
Patient isasked to take deep breathing,
if the spleen is enlarged this can be
palpated with the fingers.
124.
Palpate the kidneys
Kidney is palpated by bimanual method.
For palpation of the right kidney, place the
left hand posteriorly in the right loin
between the 12th rib and the right iliac crest
and lateral to erector spinal muscle.
Place the right hand horizontally anteriorly
in the right lumbar region.
Ask the patient to take deep breath and
press the right hand backward and press
the left hand forward.
125.
Kidney isnormally not palpable.
If kidney is enlarged it may be palpated
between the two hands (bimanually palpable).
The palpable kidney may be pushed from one
hand to the other, as kidney is ballotable.
Palpation of the left kidney is done in the
same way by placing the left hand posteriorly
in the loin and placing the right hand
Rebound tenderness
Pressureof palpation may elicit a painful
response in the region of the abdomen
suggesting an inflammatory lesion
underneath.
Sudden withdrawal of the palpating finger
may aggravate the painful response, which
is called rebound tenderness.
This is due to sudden movement of deeply
placed inflamed or ischemic organ resulting
in pain.
128.
Fluid thrill
Patientis laid supine.
Place one hand flat over the lumbar region
of one side.
Ask the patient to keep the side of his hand
firmly in the midline of the abdomen.
Tap the opposite lumbar region.
A fluid thrill is felt as wave in the palpating
hand laid flat in the lumbar region.
Fluid thrill is demonstrable in presence of
huge ascites.
129.
Shifting dullness
Patientis asked to empty the bladder and is
laid supine in the bed.
Palpate for any swelling in the abdomen.
If a swelling is present avoid percussing
over the swelling.
Start percussion from below the xiphoid to
the symphysis pubis.
Then percuss from the center of the
abdomen toward the flank on one side and
130.
mark the pointfrom where the note is dull.
Percuss from the center of the abdomen to
the other flank and mark the point from
where it is dull. The area of dullness on
both flanks are marked out.
Turn the patient to right side and wait for a
few seconds.
Now start percussing from the left flank
towards the right flank.
131.
The dullarea in the left flank now
becomes resonant and dullness on the
right flank is pushed more medially.
The percussion is repeated by turning
the patient to the opposite side.
Positive shifting dullness is found when
at least 1 liter of free fluid is present in
the abdomen.
132.
Minimal free fluidin the
abdomen
This can be demonstrated by Puddle
sign. Percuss around the umbilicus with
the patient in knee elbow position.
About 100 mL of free fluid should be
present for Puddle sign to be positive.
This is a very inconvenient position for
the patient and is no longer practiced.
133.
Head rising orleg rising test
(Carnett’s test).
Ask the patient to keep his hands over his
chest and ask him to lift his head and shoulder
off the pillow.
If the swelling disappears or becomes less
prominent then the swelling is intraabdominal.
If the swelling becomes more prominent or
remains the same then the swelling is parietal.
For lower abdominal swelling this can be
ascertained by leg rising test.
134.
Patient liessupine and is asked to lift
both the legs from the bed.
Interpretation is same as for head
rising test.
135.
Swelling is intraperitonealor
retroperitoneal
The intra - abdominal swelling may be
intraperitoneal or retroperitoneal.
Examine the lump in knee elbow position.
If the lump disappears or becomes less
prominent then it is a retroperitoneal
swelling.
If the lump becomes more prominent or
remains the same then it is intraperitoneal.
This is a very inconvenient position for the
patient and is usually avoided.
137.
Regions in theabdomen
Abdomen is divided into nine regions by four
lines.
Upper horizontal or transpyloric line is mid-way
between the umbilicus and xiphisternum.
Lower horizontal line is transtubercular line at
the level of two tubercles on the iliac crest.
Right vertical line is the line through the mid
point of right anterosuperior iliac spine and
138.
pubic symphysis.
Leftvertical line is the line through the
midpoint of left anterosuperior iliac
spine and pubic symphysis.
139.
Regions in theabdomen
1. Right hypochondrium
2. Epigastric region
3. Left hypochondrium
4. Right lumbar region
5. Umbilical region
6. Left lumbar region
7. Right iliac fossa
8. Hypogastrium
9. Left iliac fossa
It ishorizontally placed.
It usually moves with respiration.
Upper border is not felt.
It is dull on percussion (This dullness
continues over liver dullness above).
Fingers can not be insinuated under
right costal margin.
150.
Conditions where livergets
enlarged
1. Soft, smooth, nontender liver:
Hydrohepatosis. It is due to obstruction of
CBD causing dilatation of intrahepatic biliary
radicles.
Congestive cardiac failure.
Hydatid cyst of the liver: Here mass is well-
localised in the liver with typical hydatid thrill.
Three finger test: Three fingers are placed
over the mass widely. When central finger is
tapped fluid movement is elicited in lateral
151.
two fingers.
2. Soft,smooth, tender liver:
Amoebic liver abscess: Here liver often
gets adherent to the anterior
abdominal wall and will not move with
respiration. lntercostal tenderness,
right-sided pleural effusion are
common.
152.
3. Hard, smoothliver:
Hepatoma (HCC): Here a large, single, hard
nodule is palpable in the liver. But
occasionally there can be multiple nodules
when it is multicentric. Rapidly growing
tumour can be soft also. Hepatoma often can
also be tender due to tumour necrosis or
stretching of the liver capsule. Vascular bruit
may be heard over the liver during
auscultation. It mimics amoebic liver abscess
153.
in every respect.
Solitary secondary in liver.
4. Hard, multinodular liver:
Multiple secondaries in liver: Here hard
nodules show umbilication which is due
to central necrosis.
Macronodular cirrhotic liver.
It issmooth and soft (except in
carcinoma gallbladder).
It is mobile horizontally (side-to-side).
It moves with respiration.
It is located right of the right rectus
muscle, below the right costal margin
or below the lower margin of the
palpable liver.
It is dull on percussion.
156.
Conditions where gallbladderis
palpable
1. Soft, nontender gallbladder:
Mucocele of the gallbladder.
Enlarged gallbladder in obstructive
jaundice due to carcinoma head of the
pancreas or periampullary carcinoma or
growth in the CBD.
2. Hard gallbladder:
Carcinoma gallbladder.
3. Tender gallbladder-empyema GB.
157.
Other Masses inthe Right
Hypochondrium
Pericholecystic inflammatory mass: It is
tender, smooth, firm or soft, non
mobile, intra-abdominal mass often
with guarding.
Kidney mass arising from upper pole of
the kidney. It may be due to renal cell
carcinoma or hydronephrosis.
Palpable Left Lobeof the
Liver
It is in the epigastric region.
Its upper border cannot be felt.
It moves with respiration.
It extends towards left hypochondrium.
It is dull on percussion.
Conditions where left lobe of the liver
is palpable
Hepatoma
171.
Amoebic liverabscess in left lobe
Left lobe secondaries
Hydatid cyst of the left lobe
172.
Features of StomachMass
It is located in the epigastric region.
It moves with respiration. It is intra-
abdominal.
It is resonant or impaired resonant on
percussion.
Mass may be better felt on standing or on
walking.
Mass is often mobile, unless it gets
adherent posteriorly.
In pylorus mass, all margins are well felt
173.
which is mobilewith features of gastric
outlet obstruction.
Mass from the body of the stomach is
horizontally placed without any features of
obstruction.
Mass from the upper part of the stomach
near the OG junction causes dysphagia.
Mass from the fundus of the stomach is in
the upper part of the epigastric region
towards left side.
174.
Carcinoma stomachis nodular and
hard. It is the most common cause for
stomach mass.
Leiomyoma of stomach is smooth and
firm.
175.
Pseudocyst of thePancreas
Mass in the epigastric region.
It is smooth, soft.
It can be tender if it is infected.
It does not move with respiration.
It is not mobile.
It has got transmitted pulsation.
It is confirmed by placing the patient in
knee-elbow position.
176.
Lower borderis well felt. Upper border
is not clear. It is resonant on percussion.
Baid test As the stomach is pushed in
front, Ryle's tube when passed, can be
felt per abdomen on palpation.
177.
Cystadenocarcinoma of the
Pancreas
Mass is smooth, firm, does not move
with respiration, nonmobile, resonant
on percussion. Patient complaints of
back pain.
178.
Colonic Mass
Itis due to carcinoma of transverse
colon.
It is mobile, horizontally placed,
nodular, hard mass which does not
move with respiration.
Caecum will be dilated and palpable.
It is resonant or impaired resonant on
percussion.
Patient will be having bowel symptoms,
loss of appetite and decreased weight.
179.
Para-aortic Lymph Node
Mass
Mass in the epigastric region which is
deeply placed, nonmobile, not moving
with respiration.
It is vertically placed, above the level of
the umbilicus and resonant on
percussion.
Causes for enlargement are:
Secondaries, lymphomas or
tuberculosis.
180.
Aortic Aneurysm
Itis smooth, soft, pulsatile (expansile
pulsation which is confirmed by placing
the patient in knee-elbow position).
It is vertically placed above the level of
the umbilicus, nonmobile, not moving
with respiration and resonant on
percussion.
Enlarged Spleen
Spleenhas to enlarge three times to be
palpable clinically.
It enlarges towards the right iliac fossa
from left costal margin.
It moves with respiration, mobile, obliquely
placed, smooth, soft or firm, with a notch
on the anterior edge which is directed
downwards and inwards.
Fingers cannot be insinuated over the
upper border.
189.
"Hook sign"is positive, i.e. one cannot
insinuate the fingers under the left
costal margin.
It is dull on percussion.
190.
Left-sided Colonic Mass
It is mobile, nodular, resonant.
It does not move with respiration.
It is commonly due to carcinoma colon.
191.
Left Renal Massfrom Upper Pole
of any Cause
It has got features of renal mass.
192.
Left-sided Adrenal Mass
It does not move with respiration.
It is not mobile.
It is deeply placed mass.
Often it crosses the midline.
It is resonant on percussion.
It mimics kidney mass.
193.
Mass Arising fromthe Tail of the
Pancreas
Clinical features are same as other
pancreatic masses.
Causes are pseudocyst in tail of the
pancreas and cystadenomas.
There isfullness in the loin which is better
observed in sitting position.
Mass moves with respiration.
It is vertically placed.
It is bimanually palpable. It is ballotable.
Renal angle is dull on percussion (normally
it is resonant due to colon).
There is a band of resonance in front due to
reflected colon.
It does not cross the midline.
200.
Conditions Where KidneyGets
Enlarged
Hydronephrosis:
It is smooth, soft, lobulated, nontender
mass, nonmobile.
Pyonephrosis:
History of throbbing pain in the loin,
pyuria and fever with chills.
It is smooth, soft and tender kidney
mass, nonmobile.
201.
Polycystic kidney:
Historyof loin pain and haematuria.
Hypertension, anaemia and features of
renal failure.
Usually bilateral.
But one side can present early than on
the other side.
Lobulated smooth surface.
202.
Renal cell carcinoma:
History of mass in the loin, haematuria,
fever and dull pain.
Mass is nodular and hard.
It does not cross the midline.
Initially mobile; eventually it infiltrates
gets fixed and becomes non mobile.
203.
Mass from theAscending Colon on
Right Side or Descending Colon on
Left Side
History of altered bowel habits with
decreased appetite and weight.
Mass is nodular, hard which does not
move with respiration and is not
ballotable.
It is resonant or there is impaired
resonance on percussion.
Renal angle is resonant.
Proximal dilated bowel may be
palpable.
204.
Adrenal Mass
Itis nodular and hard. It does not move
with respiration.
It is not mobile and often crosses the
mid line.
It is felt on deep palpation.
It is resonant in front.
It is not ballotable.
205.
Retroperitoneal Tumours
Theyare not mobile, resonant and do
not fall forward in knee-elbow position.
They are deeply placed mass which are
usually smooth and hard.
They may be retroperitoneal sarcomas
or teratomas or lymph node mass.
206.
Retro peritoneal Cysts
They are smooth and soft with the
same features as retroperitoneal
tumours.
208.
Cystic lesions inthe
abdomen
Mucocele/empyema of gallbladder
Pseudocyst of pancreas
Ovarian cyst
Omental cyst
Aneurysm
Retroperitoneal cyst
Cystadenocarcinoma of ovary
Hydatid cyst of liver
Congenital nonparasitic cyst of liver
USUAL MASSES
Mesentericcyst
Omental cyst
Ovarian cyst (pedunculated)
Small bowel tumours
Extension of masses from other region
Transverse colon mass
Mass in the body of pancreas
Mesentery mass
Lymph node mass: secondaries (primary
from
Mesenteric cyst
Tillauxtriad:
1. Soft intra-abdominal umbilical mass.
2. Mobile in the direction perpendicular
to the attachment of the mesentery.
3. Resonant mass.
May precipitate intestinal obstruction,
volvulus.
214.
Omental cyst
Itis smooth, soft and nontender
It moves with respiration.
It is mobile in all directions
It is dull on percussion.
lntussusception
Mass inumbilical region usually towards
left and above the umbilicus.
Occasionally towards right side.
Mass is intra-abdominal which is sausage
shaped, with concavity towards umbilicus,
well-defined, smooth, firm and mobile.
Mass does not move with respiration.
Mass contracts under palpating fingers.
Often mass disappears and reappears.
217.
Mass isresonant or there is impaired
resonance on percussion.
"Red currant jelly" stool with features of
intestinal obstruction may be present.
Actinomycosis
Crohn'sdisease
Iliac artery aneurysm
Ovarian swelling-ovarian cyst
Tubo-ovarian mass
Uterine mass like pedunculated fibroid
226.
Appendicular mass
Itis smooth, firm, tender mass in the
right iliac fossa.
It is not mobile.
It does not move with respiration.
It is resonant on percussion.
It is well-localised mass with distinct
borders.
227.
Appendicular abscess
Itis smooth, soft, tender and dull mass
in the right iliac fossa with indistinct
borders.
228.
Carcinoma caecum
Itis nodular, hard, mass in the right iliac
fossa.
It does not move with respiration.
It is mobile but mobility may be
restricted once it gets adherent to
psoas muscle.
Mass is resonant or there is impaired
resonance on percussion.
Often features of intestinal obstruction
may be present.
229.
Ileocaecal tuberculosis
Massin the right iliac fossa which is
smooth, hard, resonant and nontender.
It does not move with respiration and
has restricted mobility.
Caecum may be pulled up to lumbar
region due to fibrosis.
230.
Amoeboma
History ofdysentery with pain in the
right iliac fossa.
Smooth, hard, well-defined mass in the
right iliac fossa which is nonmobile.
It may or may not be tender.
231.
Psoas abscess
Itis localised, smooth, soft, non mobile
mass in the right iliac fossa.
Psoas spasm (flexion of the hip joint) is
typical.
Spine may show gibbus, tenderness,
paraspinal spasm.
Spinal movements will be restricted.
239.
MASS IN THELEFT ILIAC
FOSSA
Carcinoma sigmoid or descending
colon
Bony masses
Ovarian/uterine masses
Psoas abscess
Ectopic kidney
Lymph node mass
Undescended testis
Bladder mass
Itis in the midline.
It is dull on percussion.
Lower border is not felt
It can be mobile in horizontal direction.
Mass reduces in size after emptying the
bladder.
It can be felt on per-rectal examination.
It is either carcinoma bladder
(common) or leiomyoma or sarcoma
bladder.
243.
Uterine mass
Itis midline mass which is smooth,
hard.
Lower border is not felt which extends
into the pelvis.
It is felt on pervaginal examination.
244.
Ovarian mass
Pelvicsoft tissue mass.
Blaxland ruler test (Athelstan J
Blaxland): A flat ruler placed on the
lower abdomen just above the
anterosuperior iliac spines and pressed
firmly backwards. In ovarian cyst, aortic
pulsation is transmitted to fingers
through ruler; it is not so in ascites.
245.
In alllower abdomen masses P/R
and/or P/V is a must.
In all regions parietal masses can occur:
Benign and malignant soft tissue
tumours; Common, is lipoma;
Fatty hernia of linea alba
Desmoid tumour
Parietal wall abscess.