Downloaded 124 times




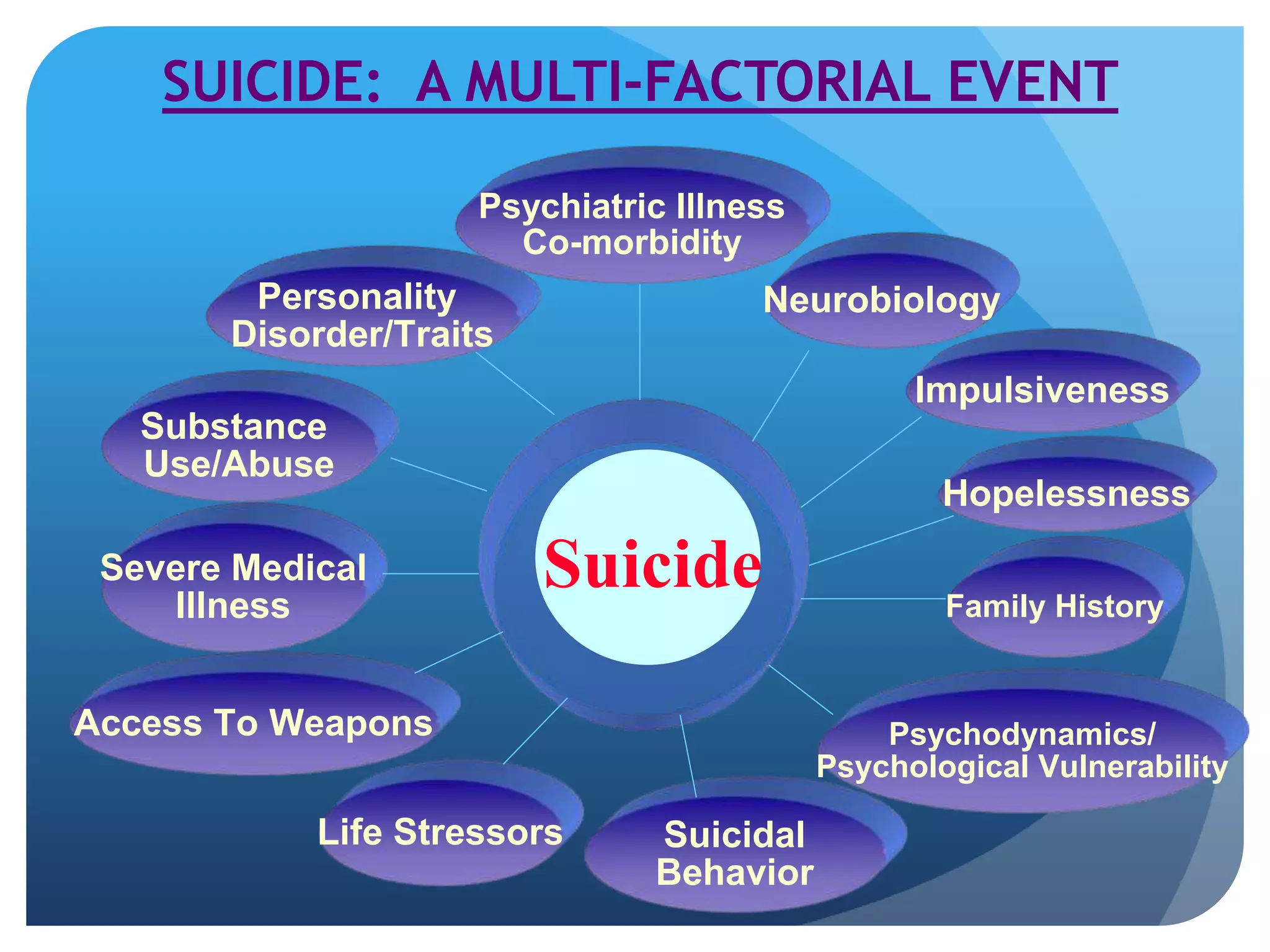

















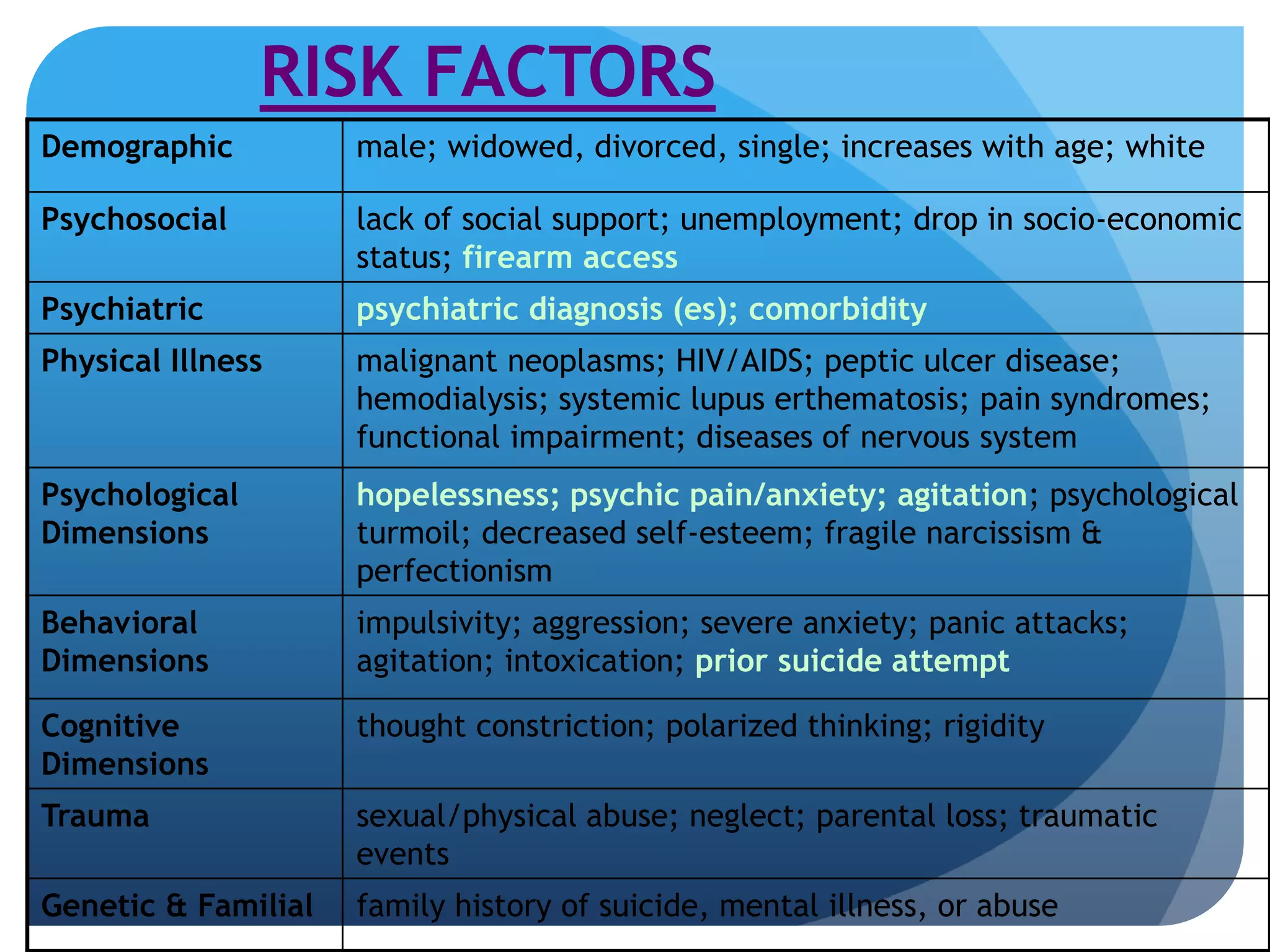






















This document defines various terms related to suicide and discusses suicide from epidemiological, etiological, and clinical perspectives. It notes that over 90% of suicides are associated with psychiatric disorders like depression and substance abuse. Key risk factors include male gender, older age, social isolation, impulsivity, and a family history of suicide. A comprehensive suicide assessment evaluates psychiatric illnesses, risk and protective factors, and determines the level of risk to guide treatment and safety planning.



















































![S U I C I D E F I N A L Original[1]](https://cdn.slidesharecdn.com/ss_thumbnails/suicidefinaloriginal1-090515122456-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


































