Downloaded 109 times


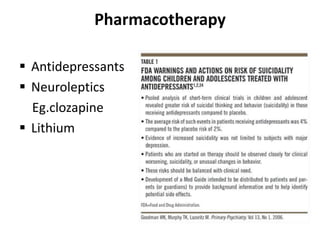





This document provides an overview of suicide and its management. It discusses the history of attitudes towards suicide, definitions and types of suicidal behaviors. Key points include that suicide is a major public health problem globally, with risk factors including mental illness, previous attempts, and access to lethal means. Treatment involves psychosocial support and pharmacotherapy. Prevention strategies target high-risk groups and aim to reduce access to lethal methods.










































































