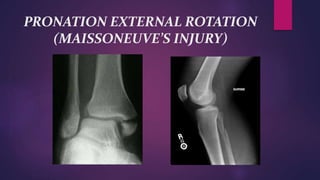
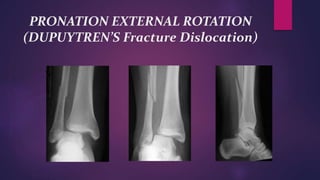
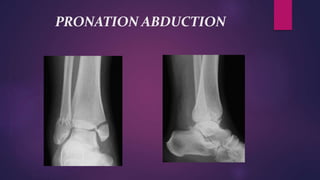
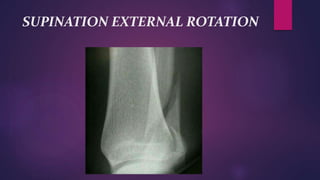
This document provides information on various ankle injuries and their management. It begins with an introduction to ankle injuries and anatomy of the ankle joint. It then describes the classification systems for ankle injuries including Lauge-Hansen and Danis-Weber classifications. Specific injury mechanisms such as supination adduction, pronation abduction, and pronation external rotation injuries are explained. Evaluation, diagnosis and treatment approaches for different types of ankle injuries like sprains, lateral malleolus fractures, and bimalleolar fractures are covered. Radiographic tests and surgical fixation options are also summarized.









































































![ANIMAL_CELL_,_TISSUE_AND_ORGAN_CULTURE[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/animalcelltissueandorganculture1-260204172026-4462b440-thumbnail.jpg?width=640&height=640&fit=bounds)


![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)












