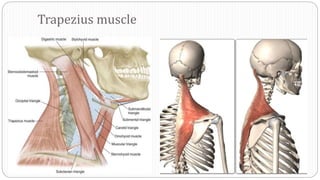
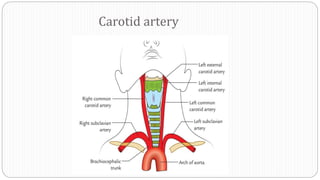
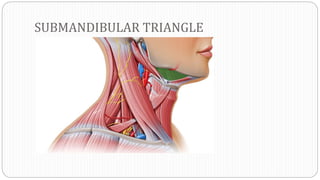
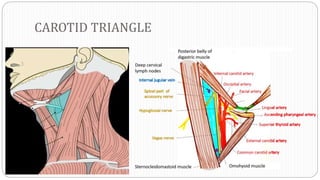
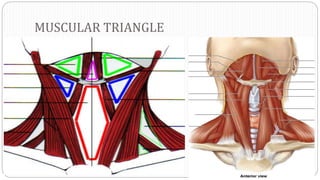
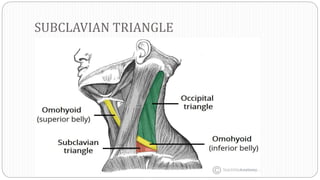
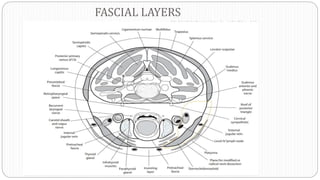
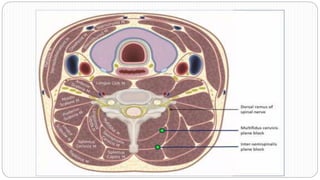
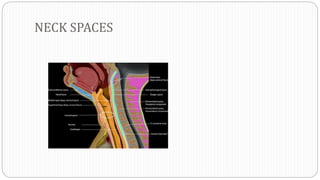
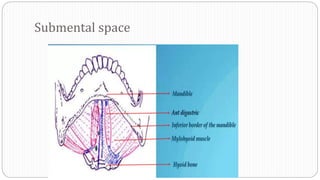
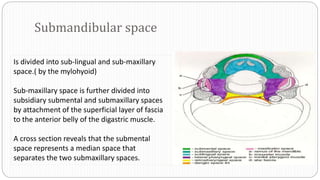
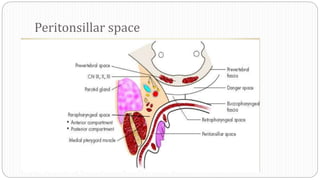
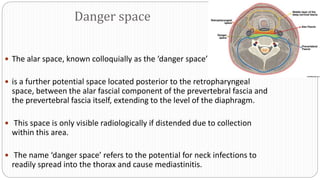
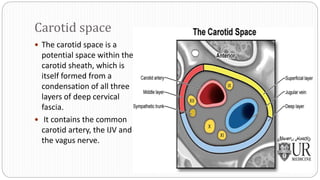
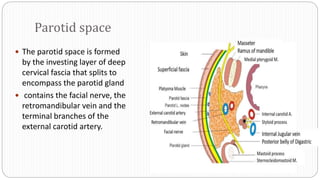
This document discusses the anatomy of the neck spaces and lymphatic system. It describes the various neck triangles and spaces, including the submental, submandibular, parotid, visceral and carotid spaces. It details the boundaries, contents and clinical relevance of infections spreading between these spaces. Important structures discussed include the carotid sheath, retropharyngeal space and danger space. The document emphasizes how neck infections can rapidly spread between spaces and threaten the airway.