Downloaded 98 times
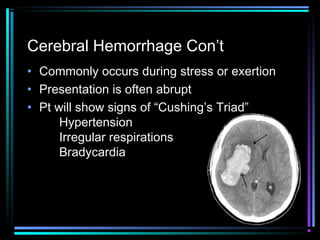
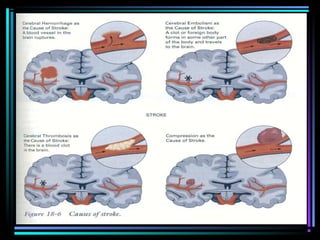


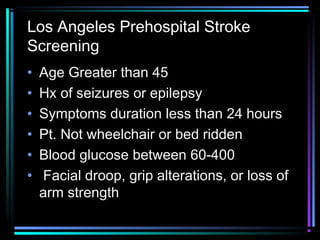
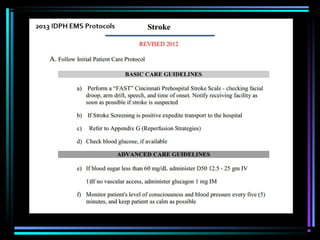

This document discusses stroke assessment for EMS providers. It defines a stroke as a sudden interruption of blood flow to the brain, outlines risk factors like hypertension and smoking, and describes common types such as thrombosis and hemorrhage. Signs and symptoms include weakness, altered mental status, and slurred speech. It emphasizes the importance of rapid assessment using tools like the Cincinnati Prehospital Stroke Scale and urgent transport to treat strokes within 3 hours of onset. Early detection and transport by EMS can significantly impact outcomes for stroke patients.























































































