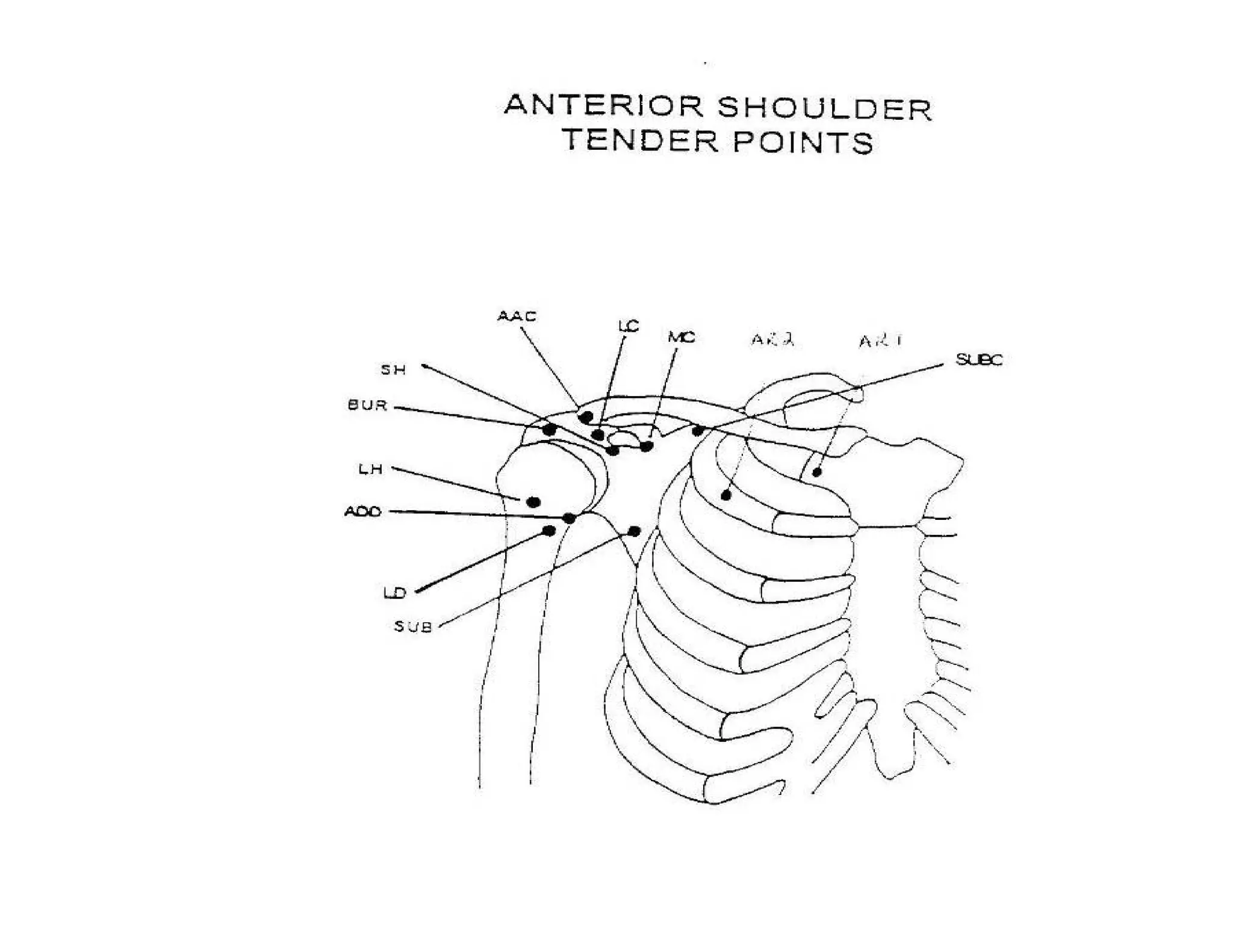
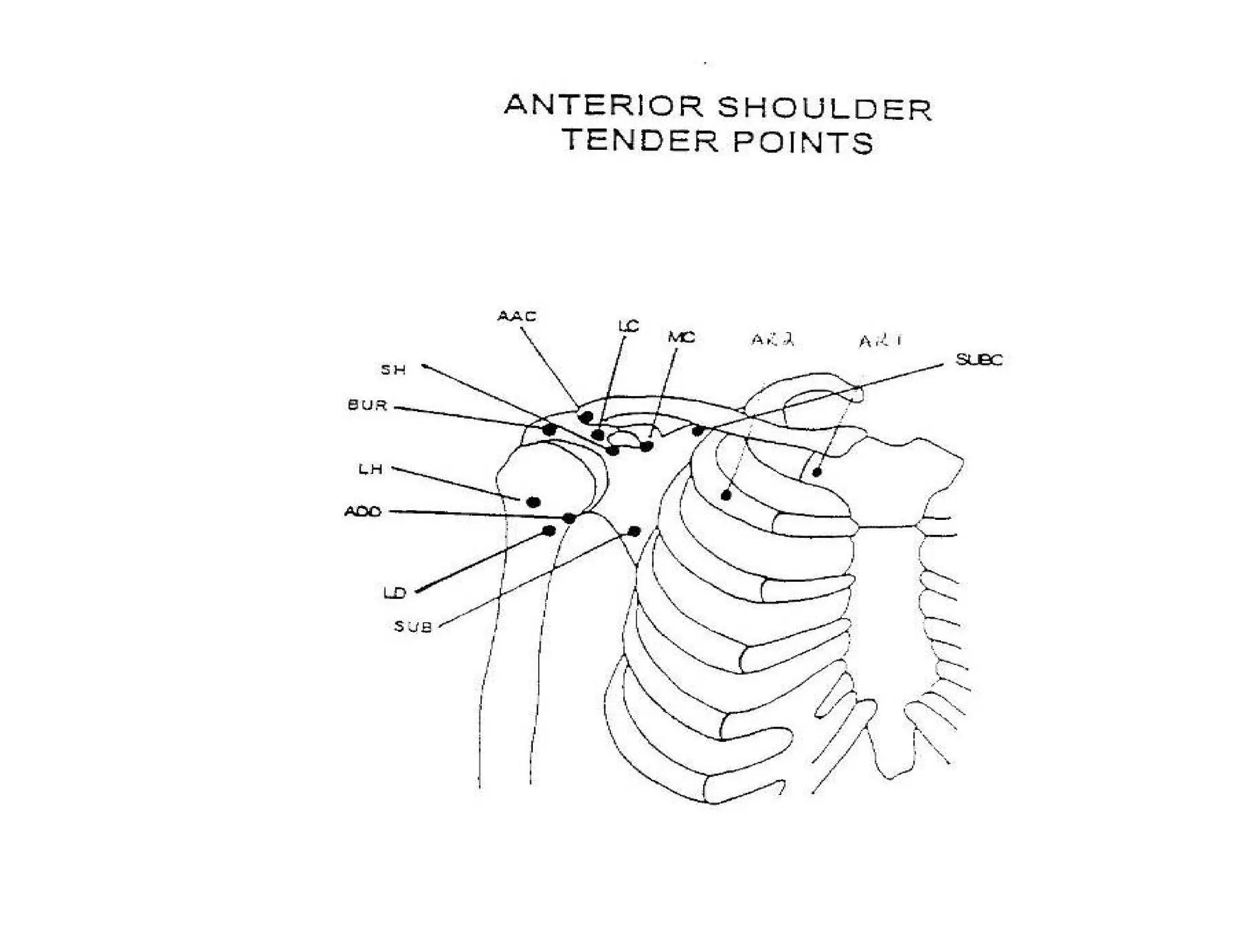
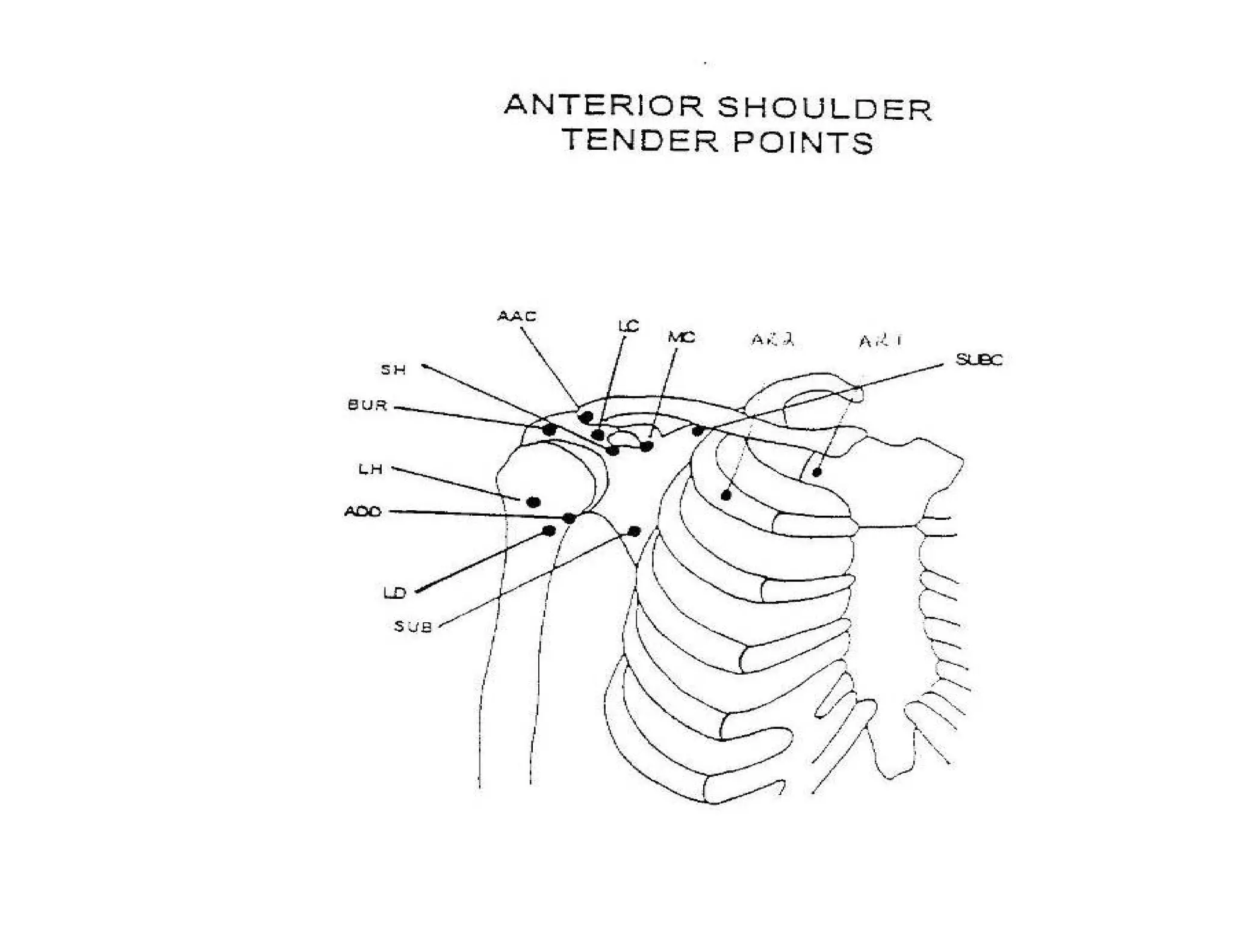
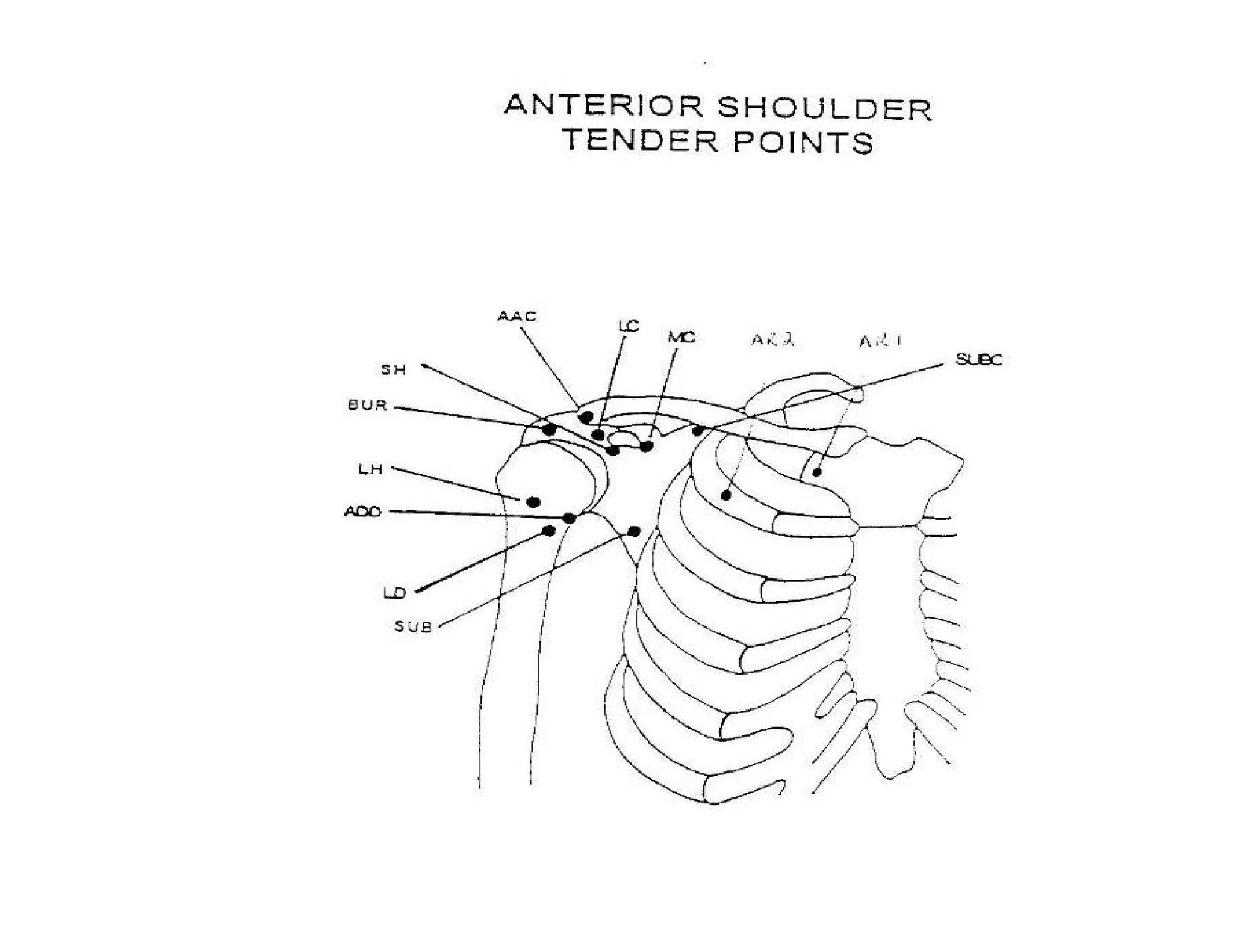
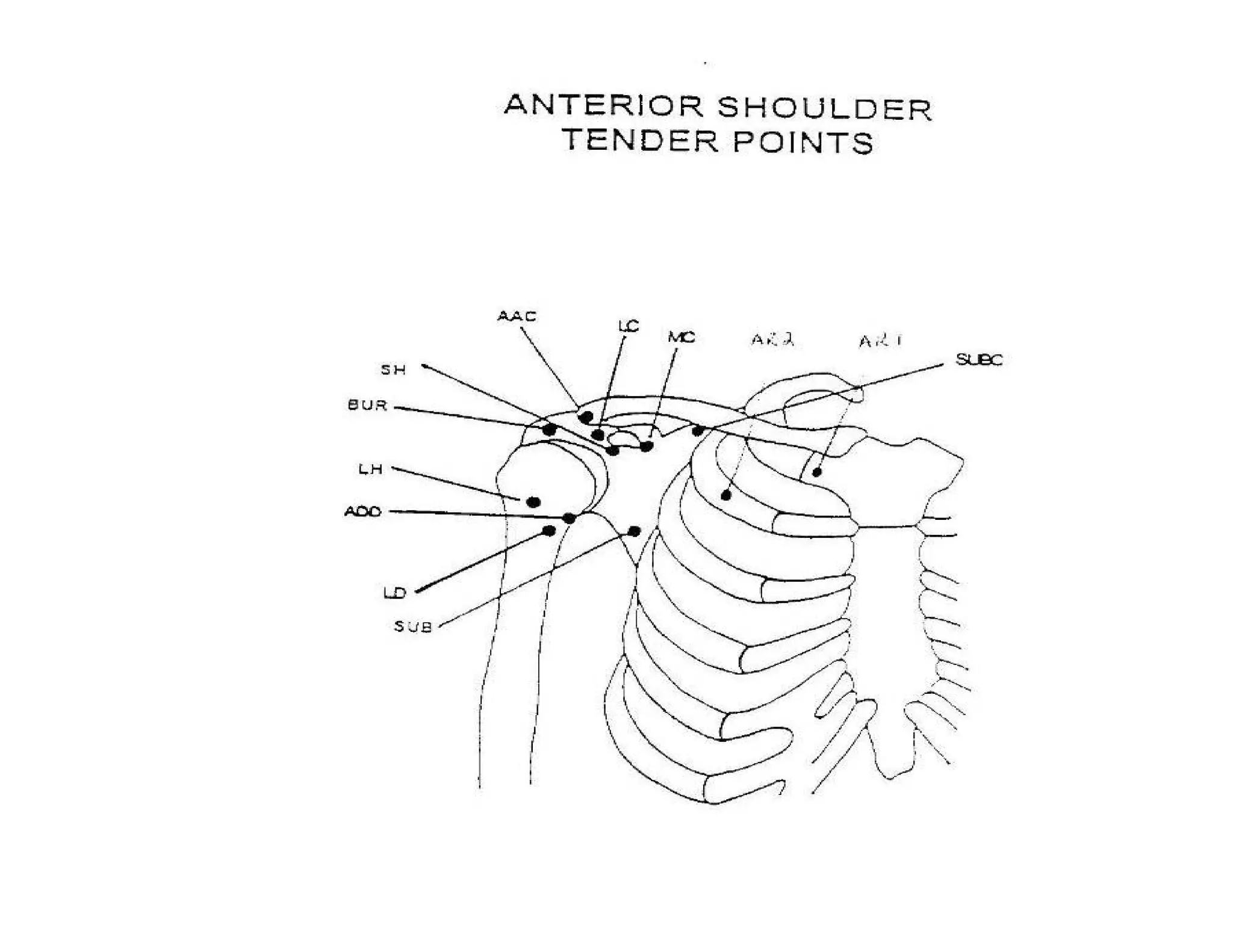
Strain-counterstrain is a manual therapy technique developed by Lawrence Jones based on the work of Irvin Korr. It involves identifying tender points associated with somatic dysfunction, finding the position of comfort for that point, and holding the position for 90 seconds to reset inappropriate proprioceptor activity maintaining the dysfunction. Over 200 distinct tender points have been identified, each with a specific positioning technique to apply counterstrain.



























































![Tip & tricks [Autosaved] - Copy.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/tiptricksautosaved-copy-220902124657-5a096dbd-thumbnail.jpg?width=640&height=640&fit=bounds)






