Downloaded 11 times



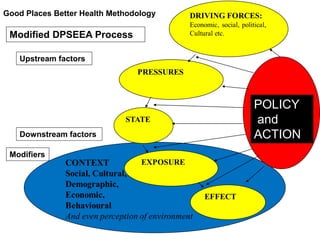
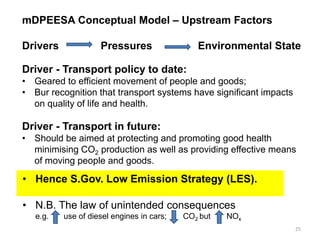
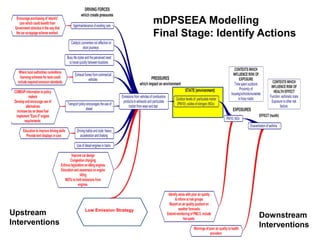

This document summarizes a presentation about a project called the Air Pollution and Health Impacts Project (APHIP). The project aims to develop evidence-based messages to encourage healthier transportation choices and reduce air pollution. It will review evidence on health effects of air pollution and strategies for changing transportation behavior. The research approach involves assessing published evidence on air pollution health impacts and behavioral change strategies using a conceptual model to identify factors influencing transportation choices and air pollution levels. The presentation outlines the rationale, questions, and intended outcomes of the APHIP project.













































































