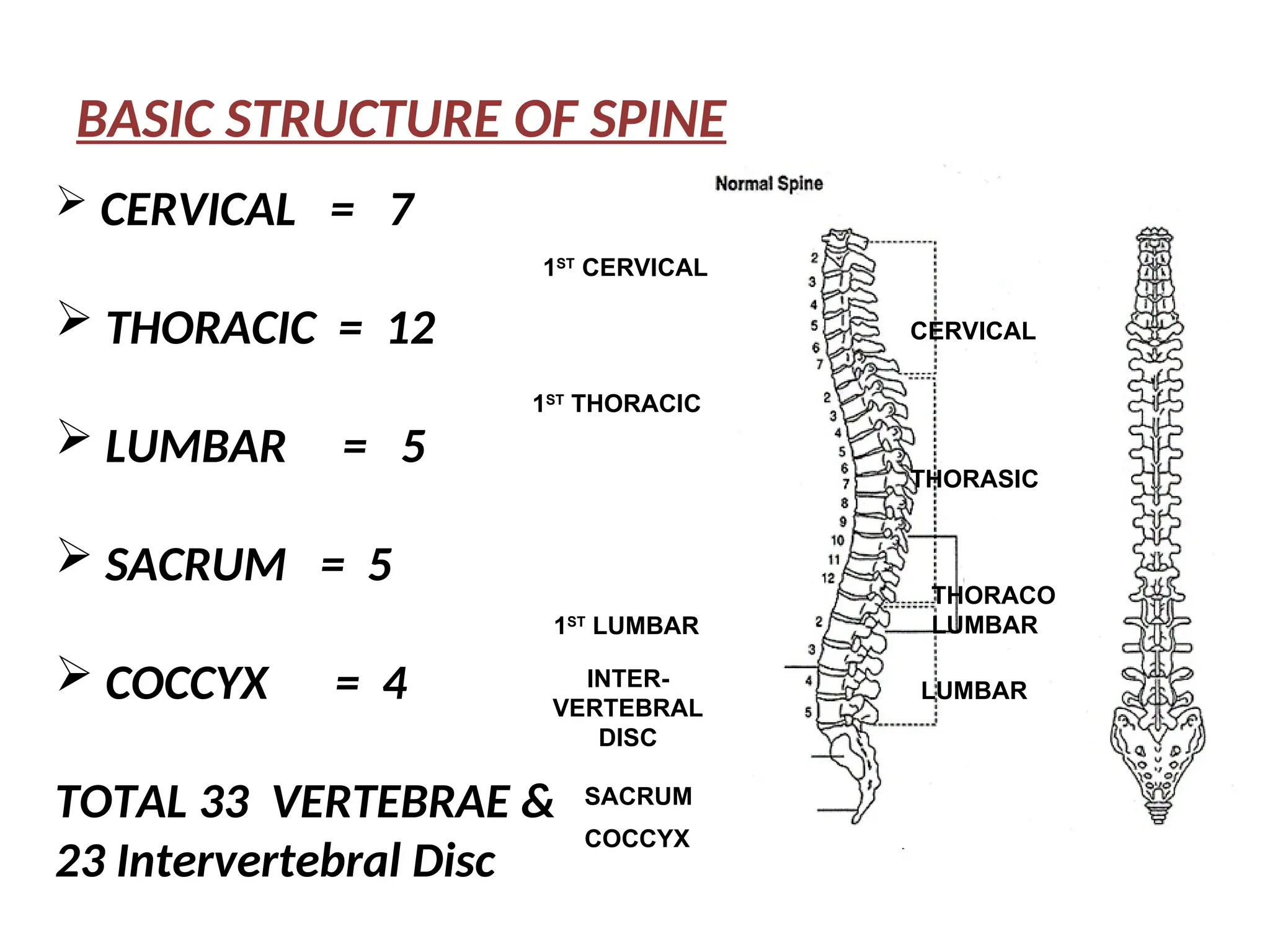
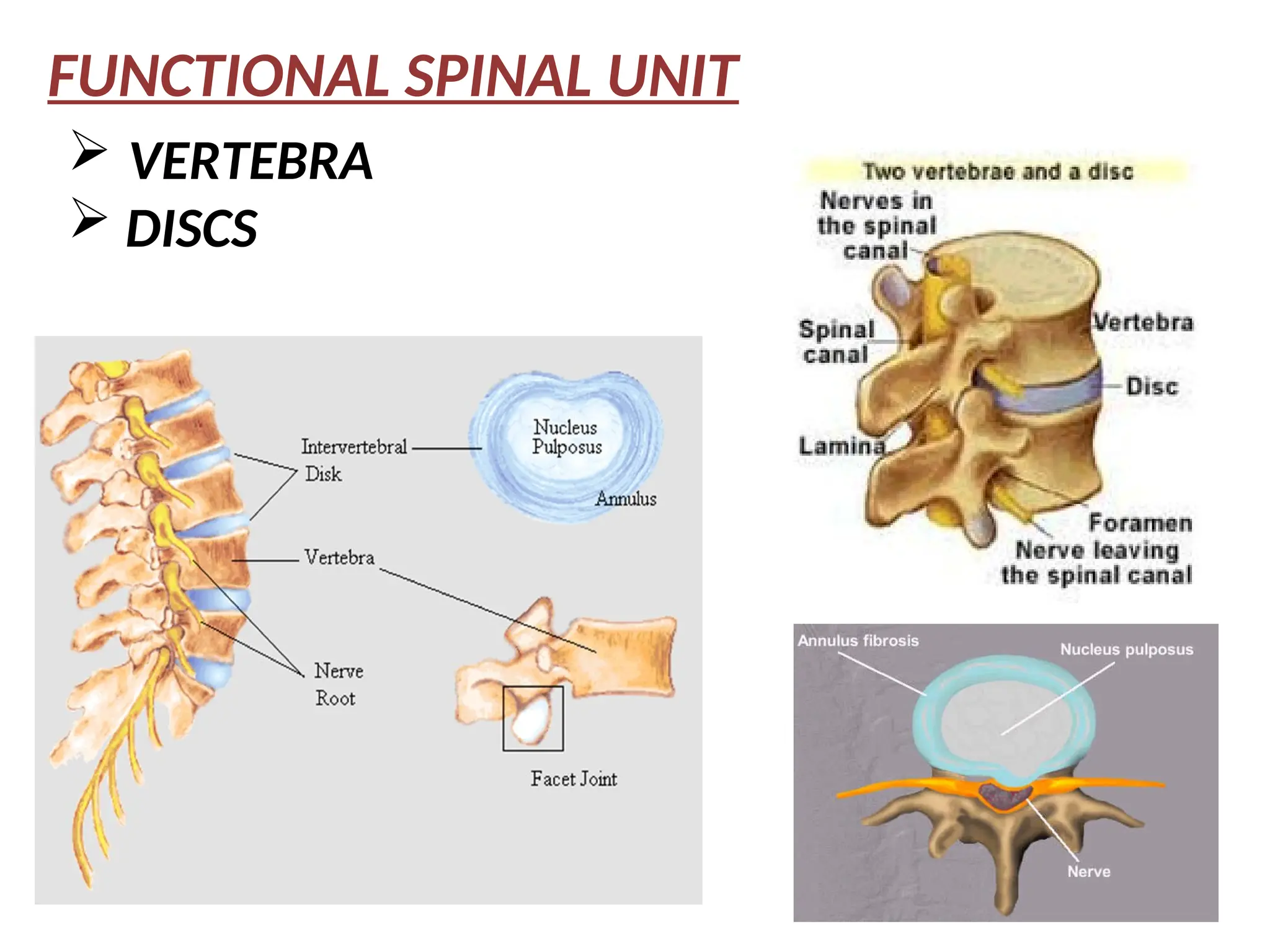
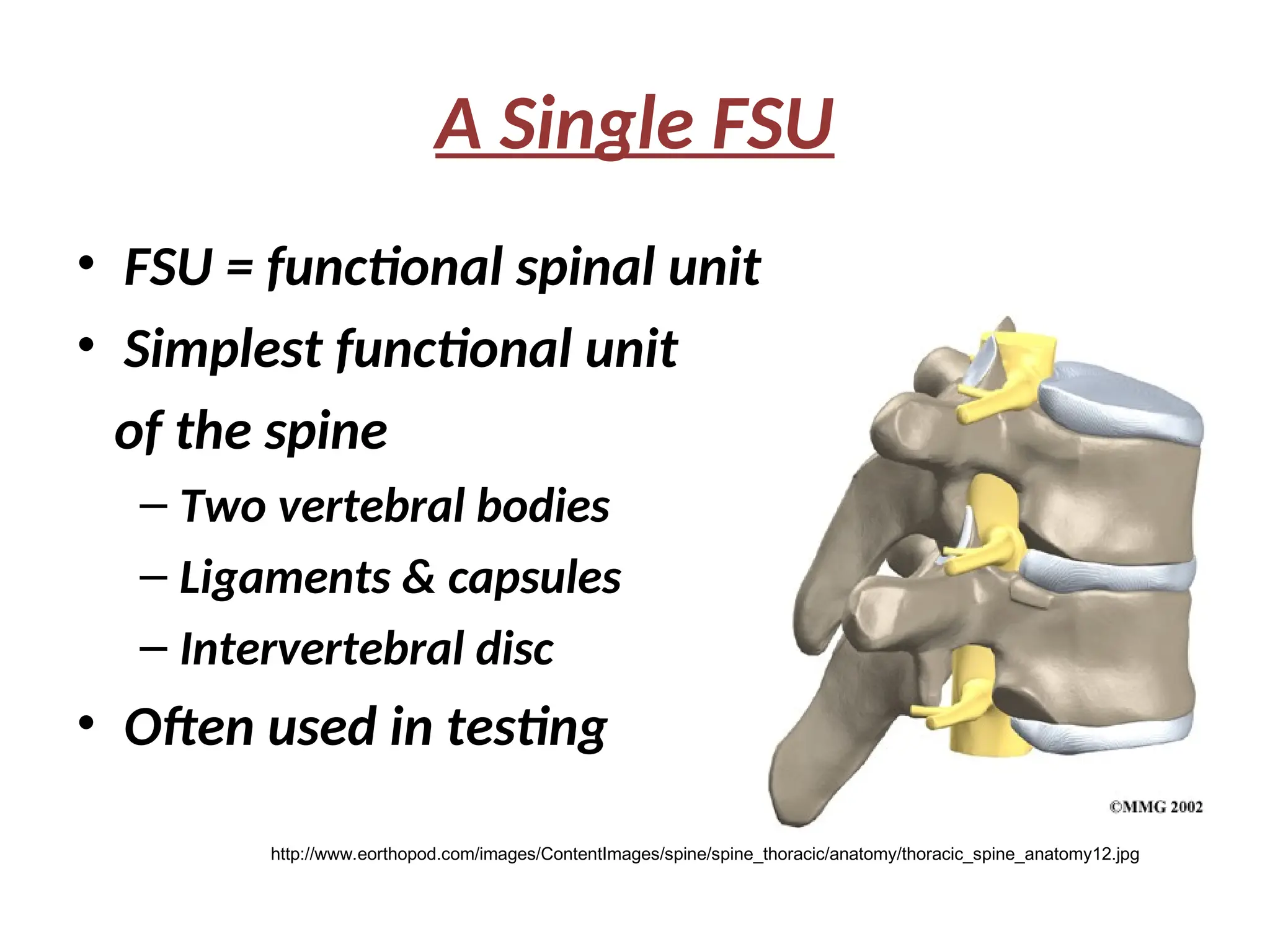
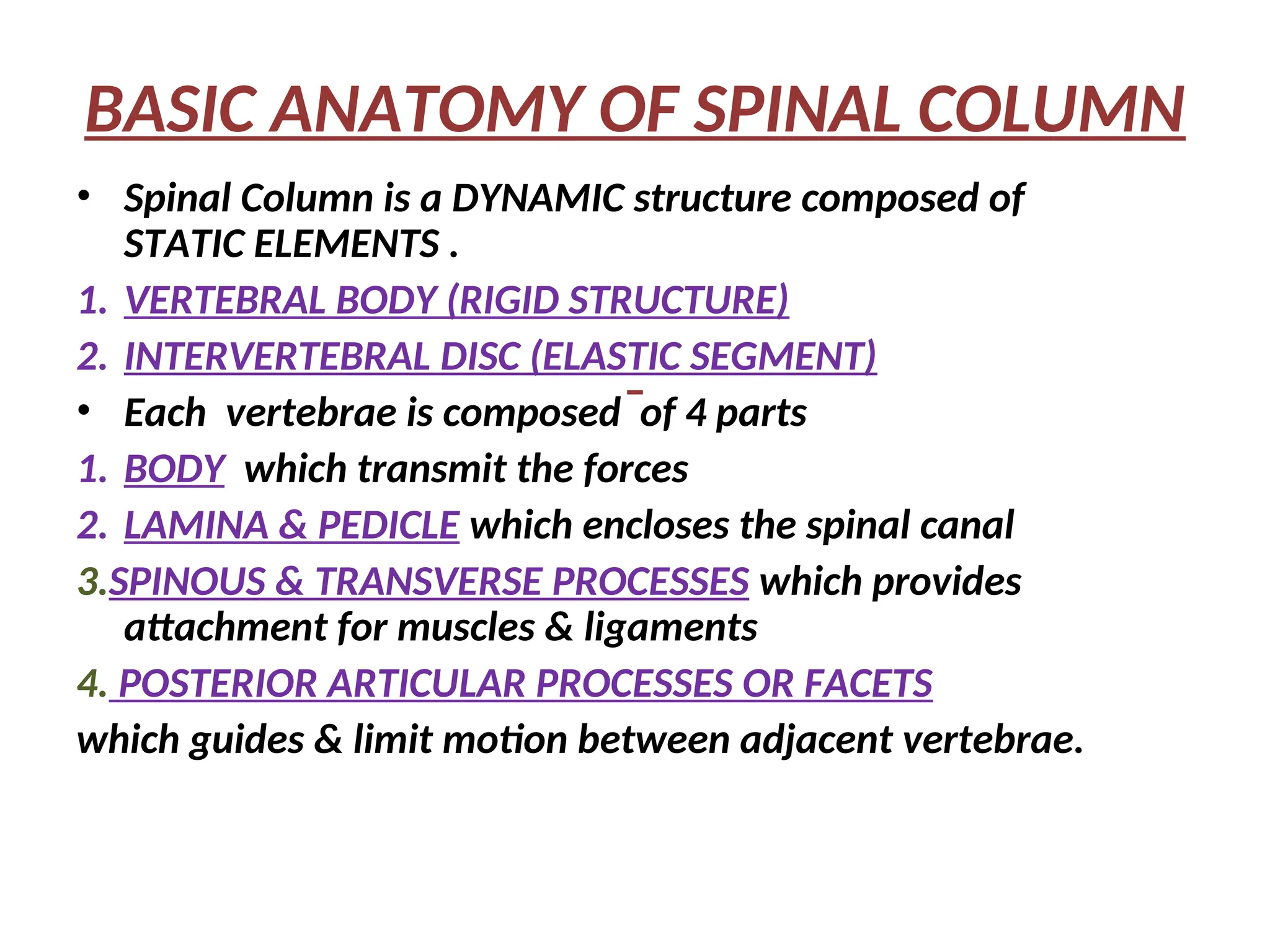
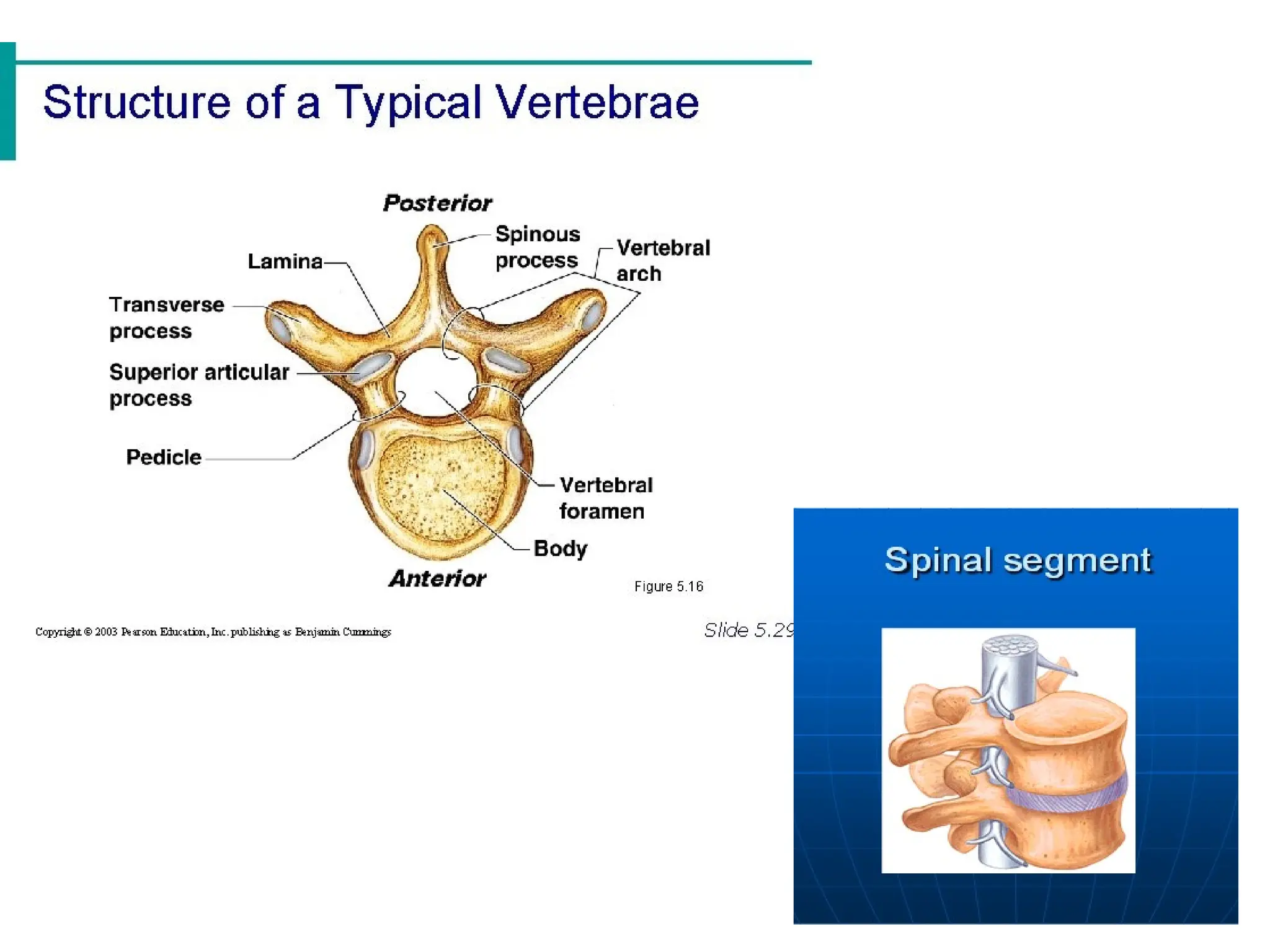
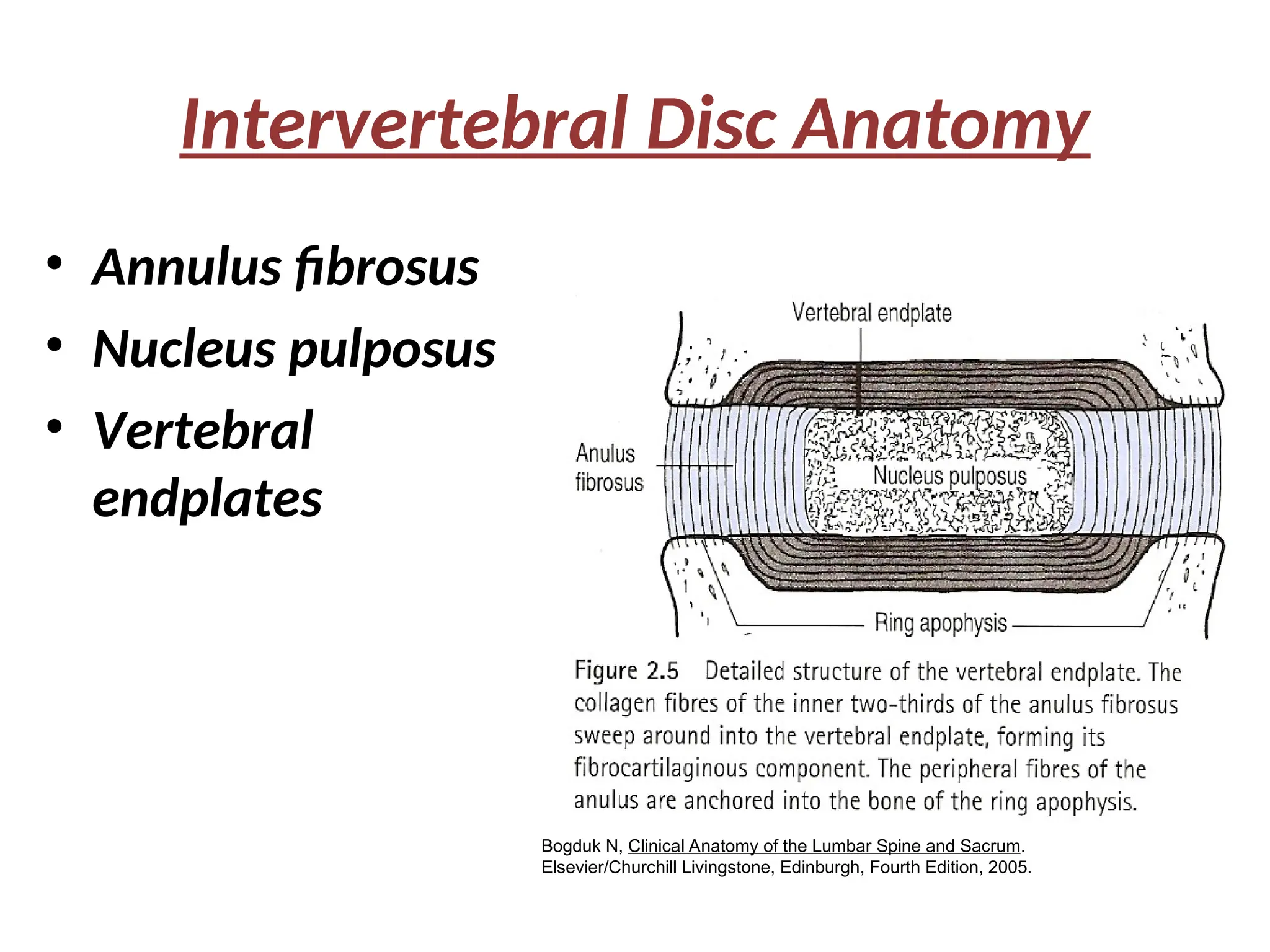
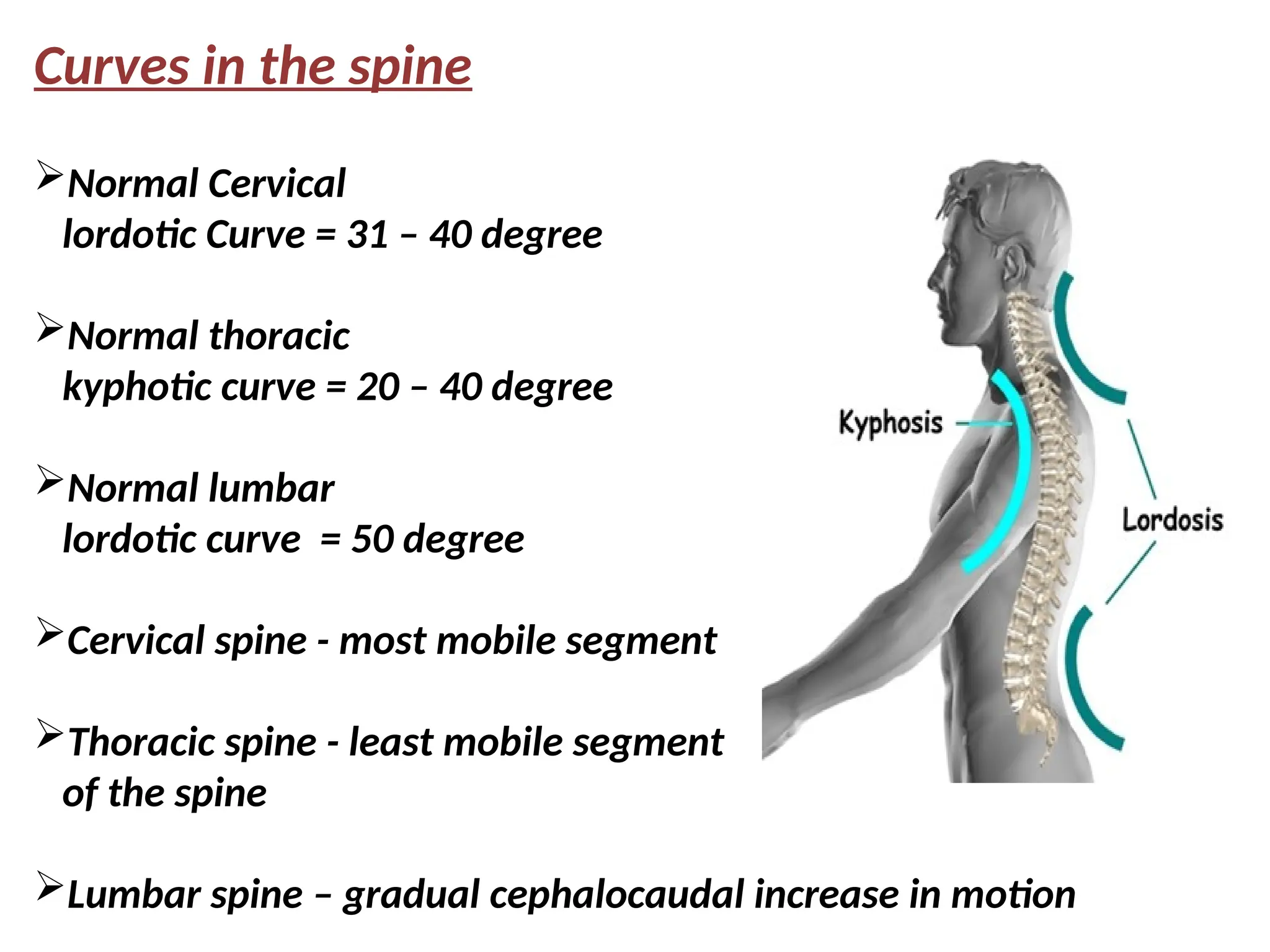
This document provides a comprehensive overview of the spinal column, including its anatomy, function, movements, and the principles of spinal orthosis. It describes the structure of vertebrae and intervertebral discs, the importance of spinal curves, and the mechanical properties of the spine. Additionally, it outlines the various indications for spinal orthosis and the associated effects, both positive and negative.