Download to read offline
![• A myotome is the group of muscles that a single spinal
nerve innervates.
• The motor level is determined by examining a key
muscle function within each of 10 myotomes on each
side of the body and is defined by the lowest key
muscle function that has a grade of at least 3 [on
manual muscle testing (MMT) in the supine position],
providing the key muscle functions represented by
segments above that level are judged to be intact
(graded as a 5 on MMT).
• This may be different for the right and left side of the
body.
Motor level
TS2_by_Shamima_2017](https://image.slidesharecdn.com/12myotome-230408052446-3e44a8f4/75/MYOTOME-pptx-2-2048.jpg)
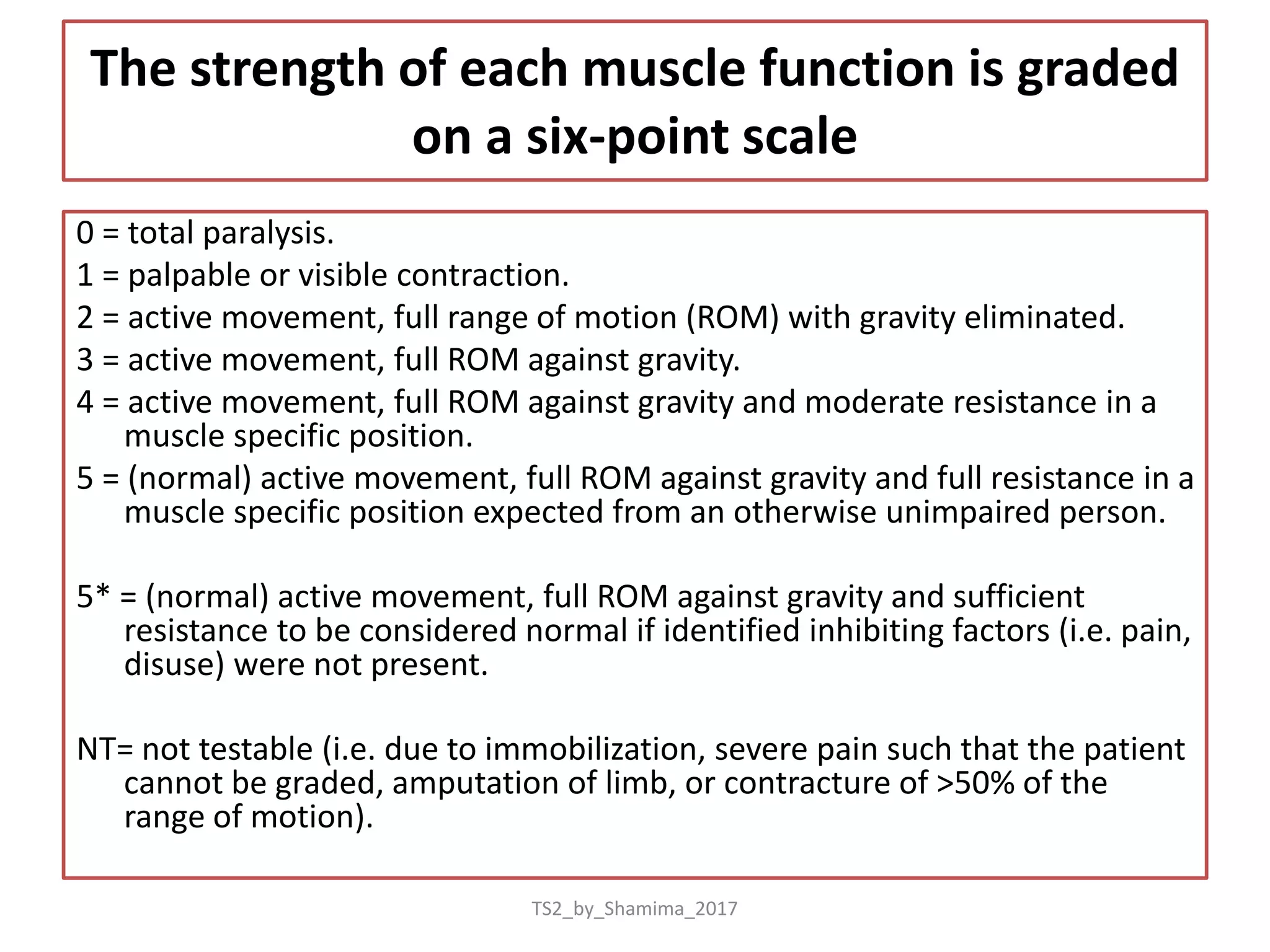

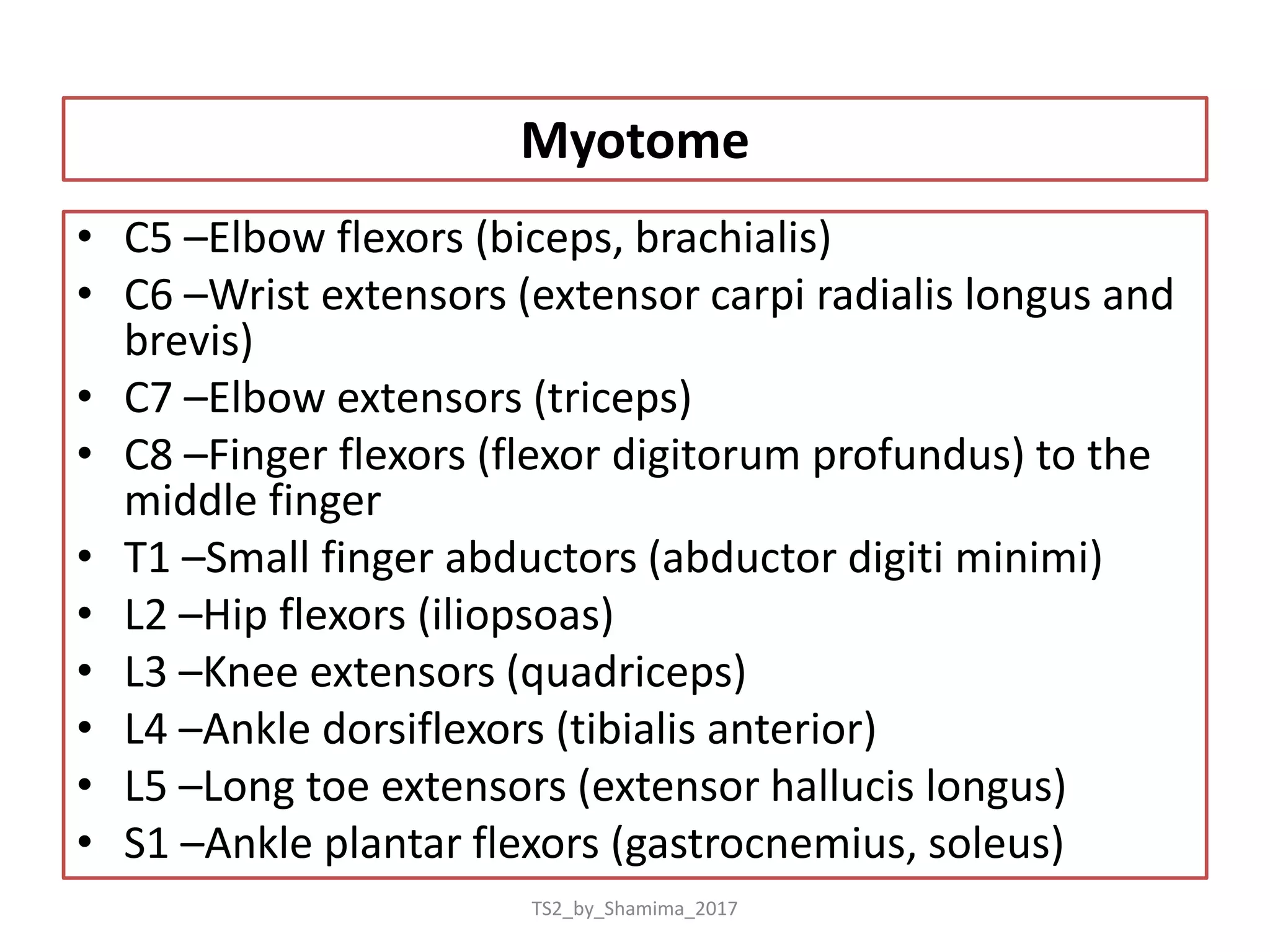


This document defines myotomes and how they are used to determine motor level after spinal cord injury. It provides the following key points: - A myotome is the group of muscles innervated by a single spinal nerve. The motor level is determined by examining 10 key muscle functions on each side and finding the lowest muscle with a strength of 3 or greater. - Muscle strength is graded on a scale of 0-5, with detailed descriptions of what each grade represents. - The document lists the specific muscles assessed for each spinal nerve level from C5 to S1 and the positioning used to test each muscle group.


















![flat foot.ppt [pes planus ] #physio.# rehabilitation](https://cdn.slidesharecdn.com/ss_thumbnails/flatfoot-240310065759-517e9bef-thumbnail.jpg?width=640&height=640&fit=bounds)