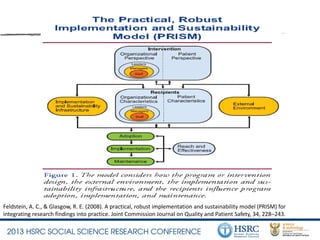
This document summarizes a family-based psychosocial intervention called VUKA for HIV-positive early adolescents in South Africa. A pilot study found high feasibility and acceptability of VUKA. A randomized controlled trial will examine VUKA's impact on behavioral, health, and psychosocial outcomes compared to standard of care. Implementation challenges include overburdened clinics, lack of counseling space/privacy, and lack of counselor support. Sustainability requires addressing organizational barriers, counselor burnout, and engaging management/government. The PRISM model will be used to evaluate factors influencing long-term adoption of VUKA.