Download as PDF, PPTX







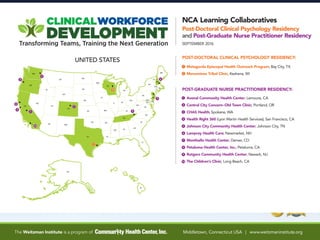







The Community Health Center, Inc. and its Weitzman Institute will provide education, information, and training to interested health centers through national webinars and learning collaboratives focused on advancing team-based care, post-graduate residency programs, and health professions students training in Federally Qualified Health Centers. The Community Health Center serves over 145,000 patients across 203 delivery sites, with a founding year of 1972. It has three foundational pillars: clinical excellence, research and development through its Weitzman Institute, and training the next generation of health professionals through various postgraduate training programs and student placements.