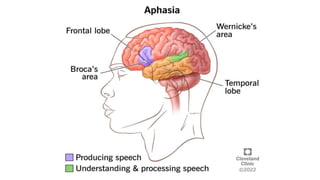
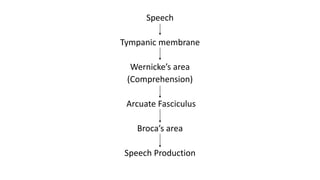
This document discusses disorders of speech. It begins by explaining the physiology of speech production, involving Broca's and Wernicke's areas of the brain. It then describes different types of speech disorders, including organic disorders affecting the brain or vocal cords, and functional disorders like stuttering. Specific disorders are explained in more detail, such as different types of aphasia resulting from brain lesions. Assessment of speech is also discussed.