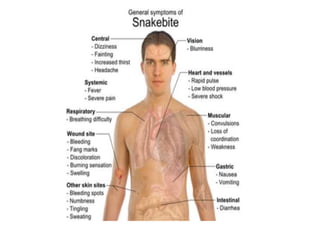
1. The document discusses snake classification, types of venomous snakes in India, signs and symptoms of snake bites, and management of snake bites.
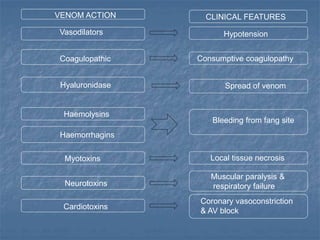
2. Poisonous snakes are classified based on the type of venom secreted into three families - Elapidae which secretes neurotoxic venom, Viperidae which secretes haemotoxic venom, and Hydrophidae which secretes myotoxic venom.
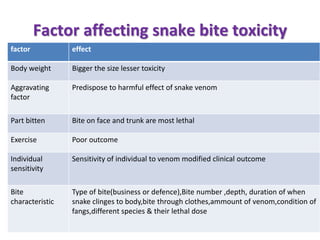
3. Common poisonous snakes in India include cobras, kraits, Russell's vipers, and sea snakes. Bites from kraits and Russell's vipers are more toxic than cobra bites.
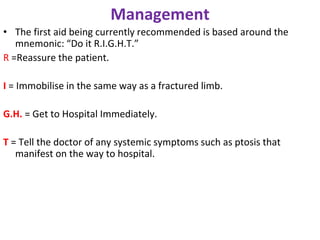
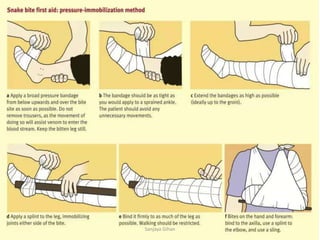
4. Management of snake bites involves local treatment, administration of antivenom, and supportive care depending




























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)













