Downloaded 2,241 times













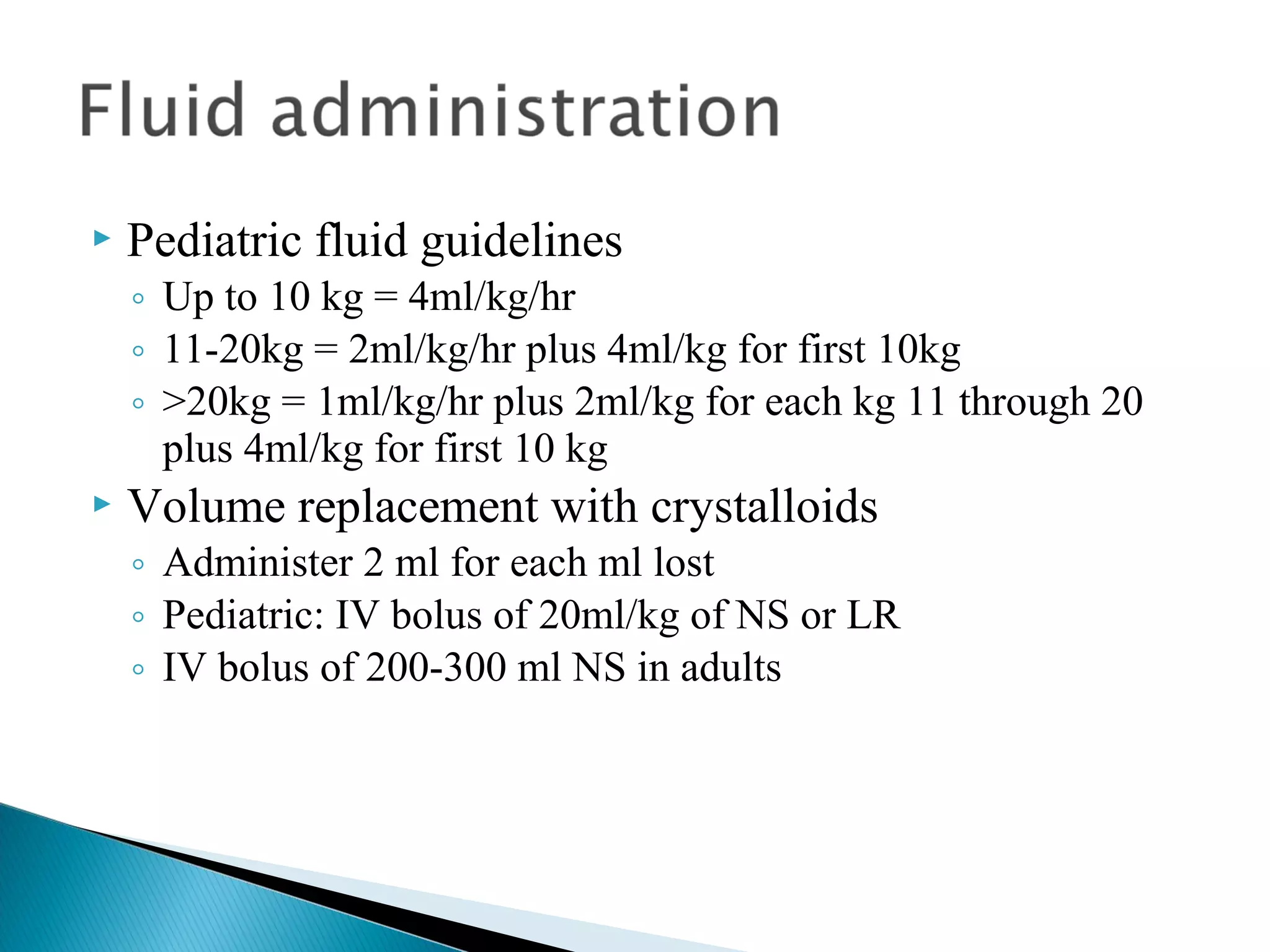














































The document provides guidance on the nursing management of shock. It discusses assessing the type and phase of shock, providing emergency nursing care, monitoring the patient closely, making a diagnosis based on history and assessments, treating with fluid resuscitation and blood products, and monitoring the patient's response. It also covers age-related considerations and the three phases of shock: compensated, uncompensated, and irreversible.



































































