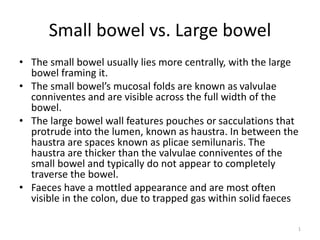
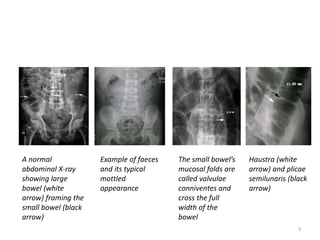
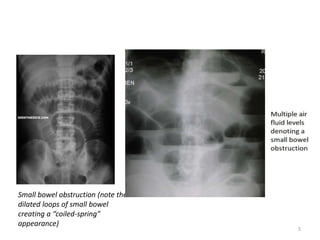
The document compares and contrasts the small bowel and large bowel. The small bowel lies more centrally and has mucosal folds called valvulae conniventes that cross its full width. The large bowel has pouches called haustra and spaces called plicae semilunaris between them. The haustra are thicker than the valvulae conniventes and do not fully traverse the bowel. Normal diameter limits are 3cm for the small bowel and 6cm for the colon, with the caecum at 9cm. Small bowel obstruction appears as dilated loops over 3cm in diameter with prominent valvulae, while large bowel obstruction shows colonic distension proximal to the obstruction and collapse







































![BF-Quiz_Abdomen-Ria,_Iqo,_Yan,_Ayu[1][1][1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/bf-quizabdomen-riaiqoyanayu111-250803152136-0c5367ce-thumbnail.jpg?width=640&height=640&fit=bounds)






































