Download to read offline























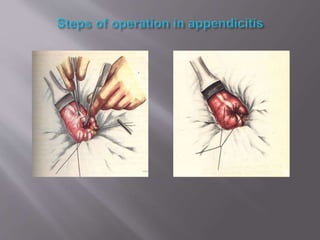

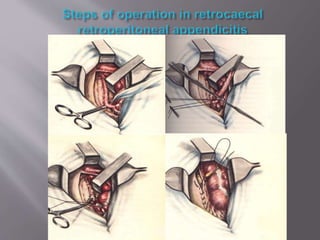








This document outlines the anatomy, pathophysiology, diagnostic considerations, and management of appendicitis, emphasizing common presentations and risk factors. It discusses imaging studies, laboratory evaluations, and differential diagnoses, providing a detailed overview for effective diagnosis and treatment. Surgical procedures for appendectomy are described step-by-step, highlighting techniques and considerations for various patient populations.