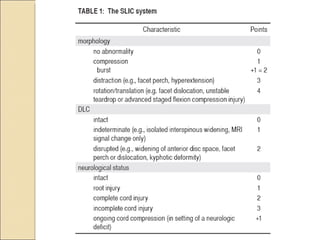
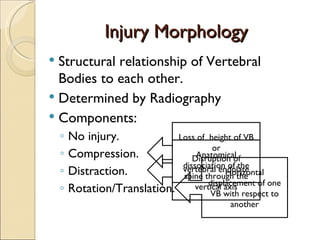
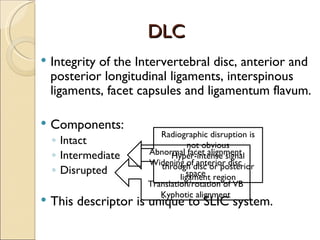
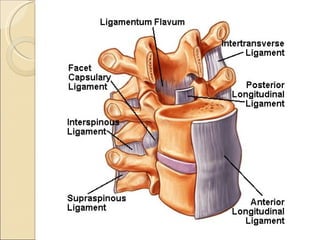
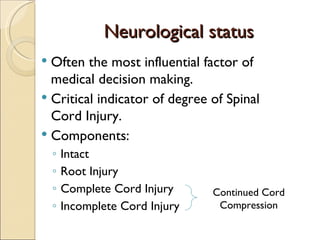
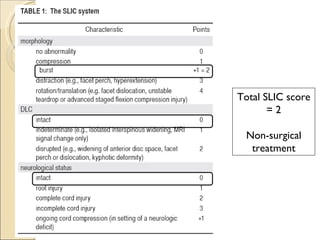
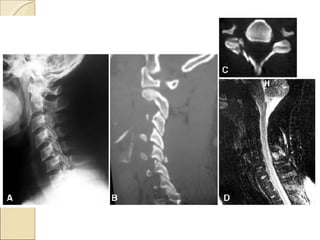
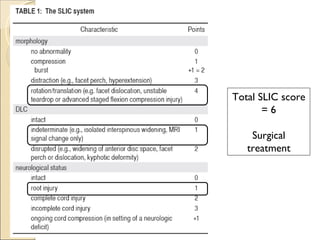
The document outlines a new classification system called SLIC (Subaxial injury classification) for cervical spine injuries. SLIC scores injuries based on 3 major components: injury morphology, integrity of ligaments and discs (DLC), and neurological status. It also includes minor descriptors. The SLIC system is demonstrated through two case examples and is compared to older classification systems. The SLIC system provides standardized treatment guidance based on total score and has shown better inter-rater agreement than prior systems. However, neurological examination and MRI interpretation introduce some subjectivity.