Downloaded 55 times
![Background
• Exclusive breastfeeding (EBF) for first six months of
life is beneficial to child and mother [1,2].
• EBF protects a child from under nutrition and
gastro-enteristis. In the long run, EBF is protective
against a number of chronic disease such as
leukaemia, type 2 diabetes, and obesity [3,4].
• Breastfeeding also has proven benefits for the
neuro-cognitive development of the child,
protection from childhood respiratory illness and
protection for the mother from breast cancer.
• EBF also saves the cost associated with illnesses
that arise out of the above mentioned illnesses [5].](https://image.slidesharecdn.com/projectmgmt-150921110103-lva1-app6892/85/Situation-Analysis-of-Project-Planning-4-320.jpg)
![Background
• For these reasons, the World Health Organization
(WHO), United Nations Children’s Fund (UNICEF)
and Ministry of Health and Population Nepal
recommend and promote exclusive breastfeeding
for first six months of life and continuation of
breastfeeding thereafter [6-8].
• Any food provided to a newborn before the
initiation of mother’s breastfeeding is considered to
be a prelacteal feed. The type of prelacteal feeds
depends on the culture. It may include ghee (refined
butter), honey, sugar, sugar juice, unboiled cow/goat
milk etc [9].](https://image.slidesharecdn.com/projectmgmt-150921110103-lva1-app6892/85/Situation-Analysis-of-Project-Planning-5-320.jpg)
![Background
• The practice of prelacteal feeding is a major cultural
practice still prevalent in many places throughout
South Asia regions [9].
• All prelacteal feeds are provided for non nutritional
reasons such as clearing the throat/bowel; or
thinking that mother’s milk is insufficient or the
colostrum is too heavy for the newborn to digest [9].
• Prelacteal feeds have lesser nutrient and
immunological value; and are often likely to
introduce contaminants [9].](https://image.slidesharecdn.com/projectmgmt-150921110103-lva1-app6892/85/Situation-Analysis-of-Project-Planning-6-320.jpg)

![Identify known barrier to behavior change
• Availability – One of the study done in Bhaktapur
district in 2012 showed that 72.3% women didn’t had
information about Breastfeeding during ANC visit.[10]
• Accessibility – Due to geographical difficulties,
unavailability of HWs, traditional home delivery
practices etc (Fifty-eight percent of mothers received antenatal care from a skilled
provider (a doctor, nurse, or midwife) for their most recent birth in the five years preceding
the survey). (NDHS 2011)
• Affordability – ANC services are provided free of cost
in government institutions. In addition they can get
incentive after institutional delivery.
• Acceptability – in most of the society of Nepal there is
practice of pre lacteal feeding before colostrum
feeding.](https://image.slidesharecdn.com/projectmgmt-150921110103-lva1-app6892/85/Situation-Analysis-of-Project-Planning-13-320.jpg)
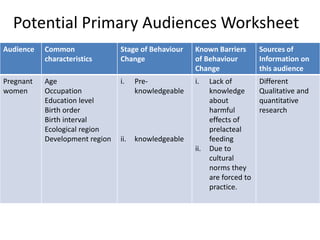
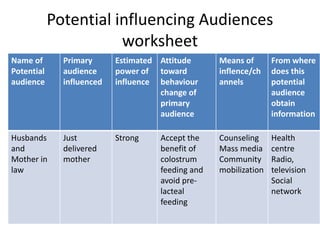
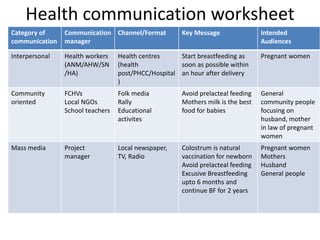
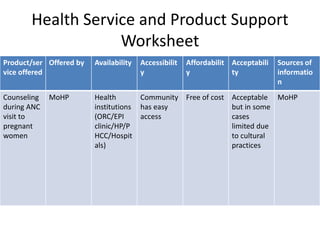
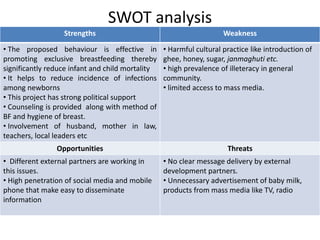


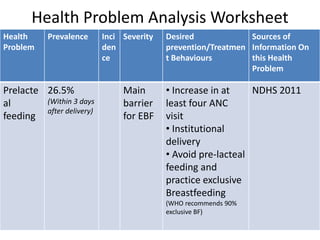
This document provides a summary of project management for reducing pre-lacteal feeding in Nepal. It begins with an analysis of the problem, identifying key audiences and communication resources. Exclusive breastfeeding is recommended but pre-lacteal feeding is still common due to cultural norms. The document identifies pregnant women as the primary audience and outlines known barriers like lack of knowledge and cultural practices. Potential communication channels are identified including health workers, community members, and mass media. An environmental analysis considers supportive health services but also threats like non-clear messaging. A SWOT analysis identifies strengths like political support but also weaknesses like cultural practices and limited access to media.

























































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)






