Downloaded 201 times











The SIGNIFY trial investigated the effects of ivabradine in 19,102 patients with stable coronary artery disease without heart failure. It found that ivabradine reduced heart rate but did not improve cardiovascular outcomes and increased adverse events compared to placebo. However, ivabradine was found to improve angina symptoms in patients who had angina at baseline. The results contrast with previous studies and suggest that reducing heart rate may not benefit stable coronary artery disease as it does heart failure.
Introduction of Ivabradine's relevance in coronary artery disease and the existing controversies.
Elevated heart rate as a cardiovascular risk; Ivabradine mechanism of heart rate reduction.
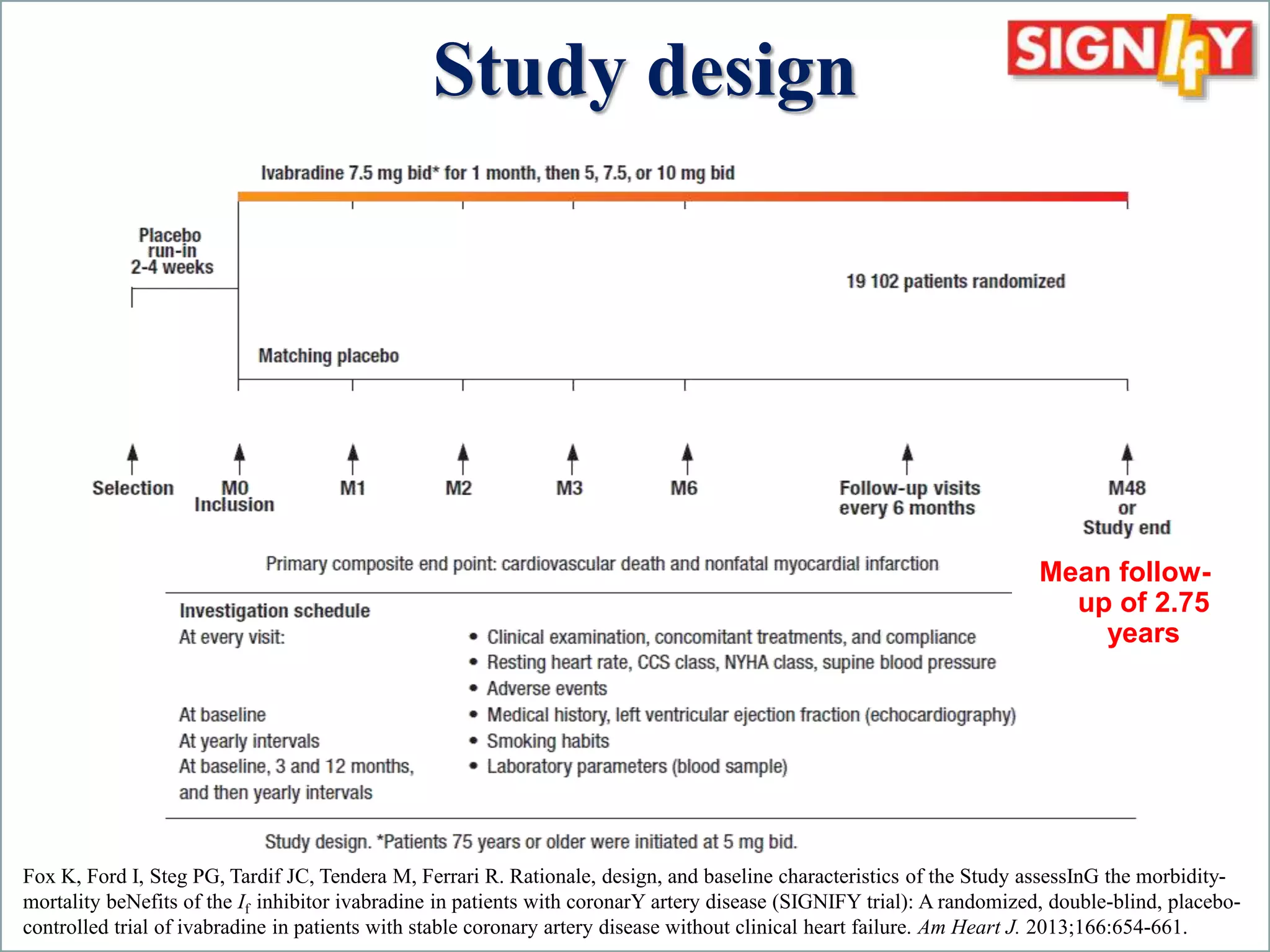
Overview of the SIGNIFY trial design, aim, and structure involving stable coronary artery disease patients.
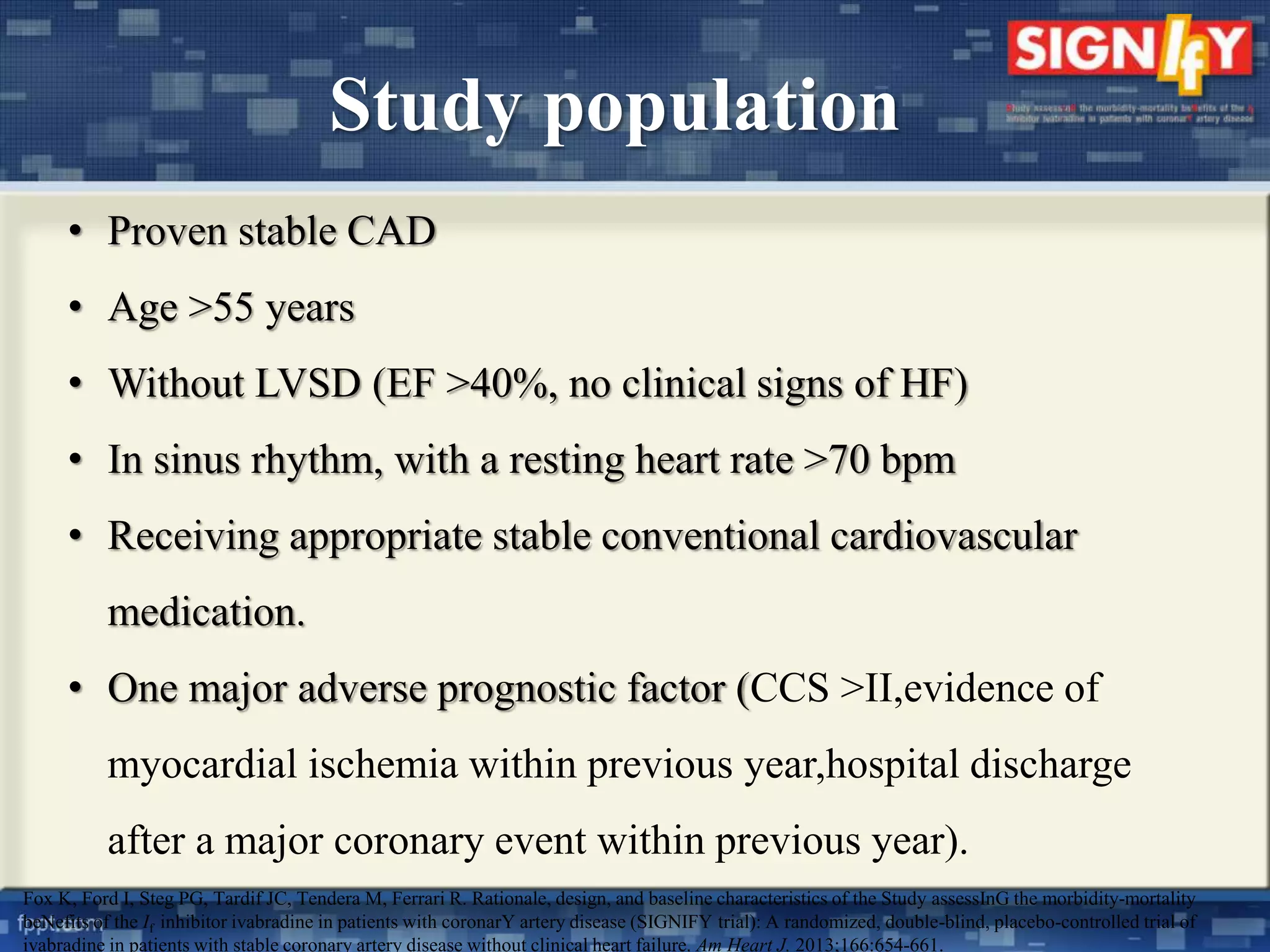
Inclusion and exclusion criteria focusing on age, heart function, and symptoms of study participants.
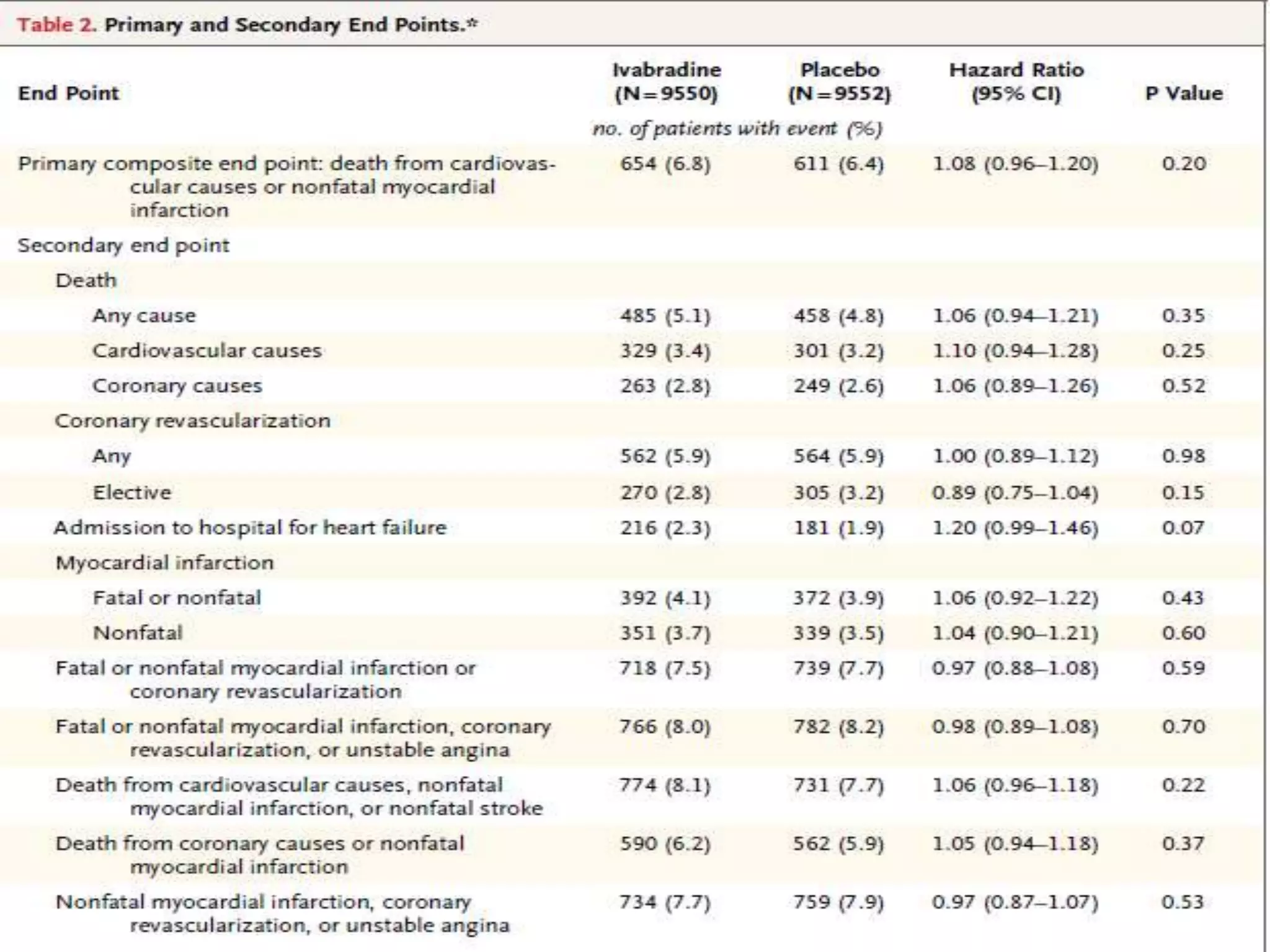
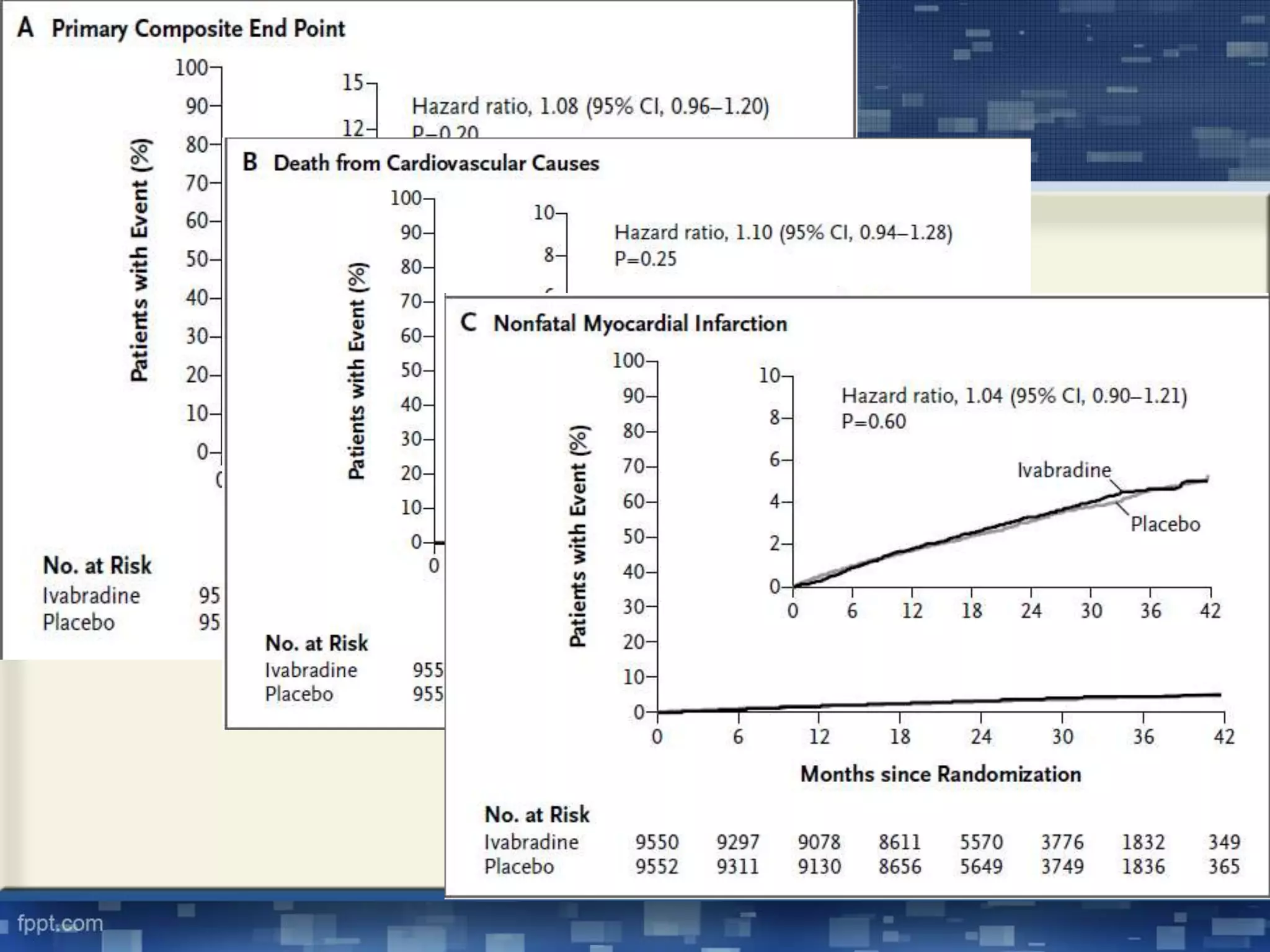
Primary and secondary endpoints of the study designed to measure cardiovascular outcomes.
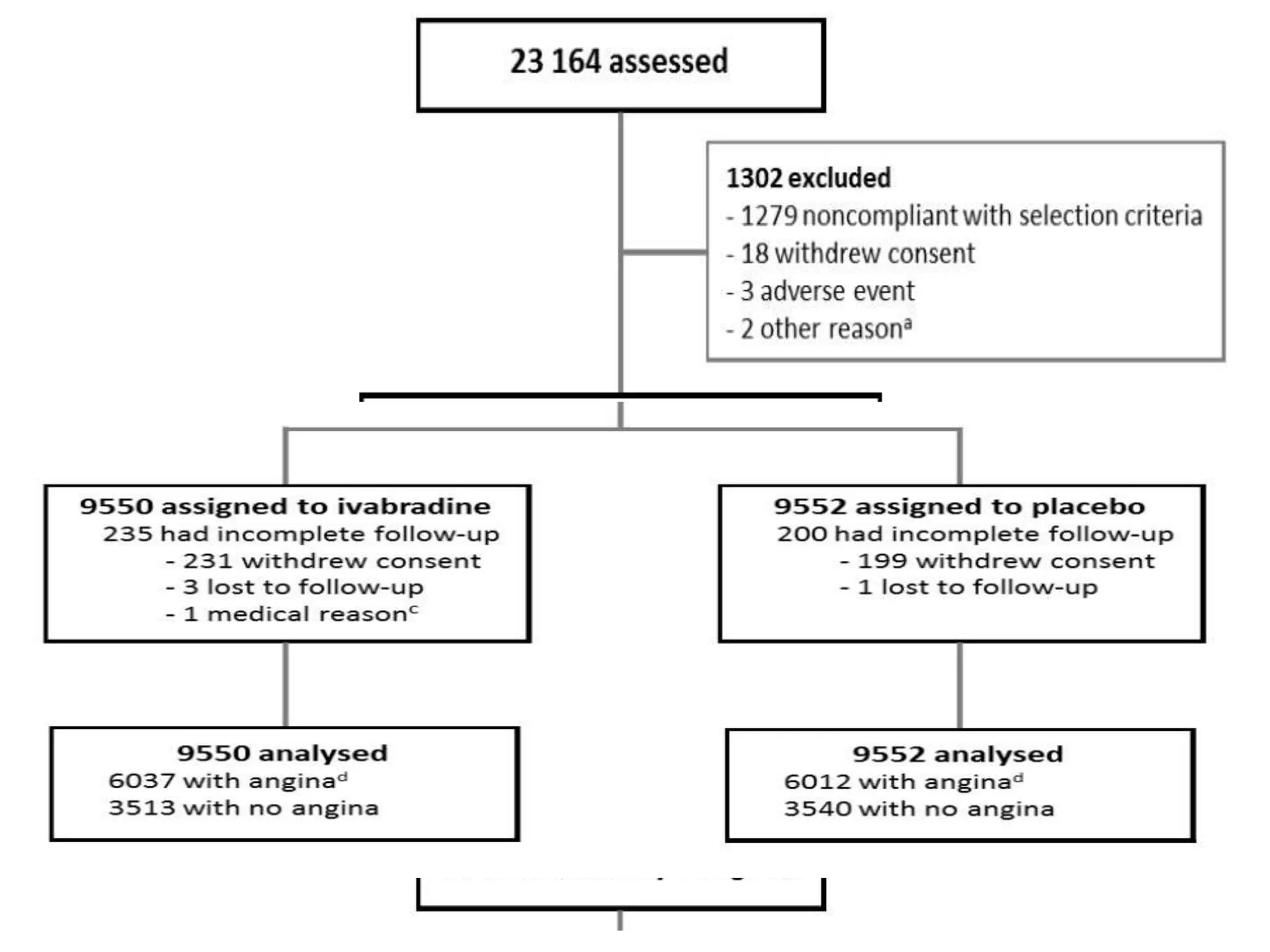
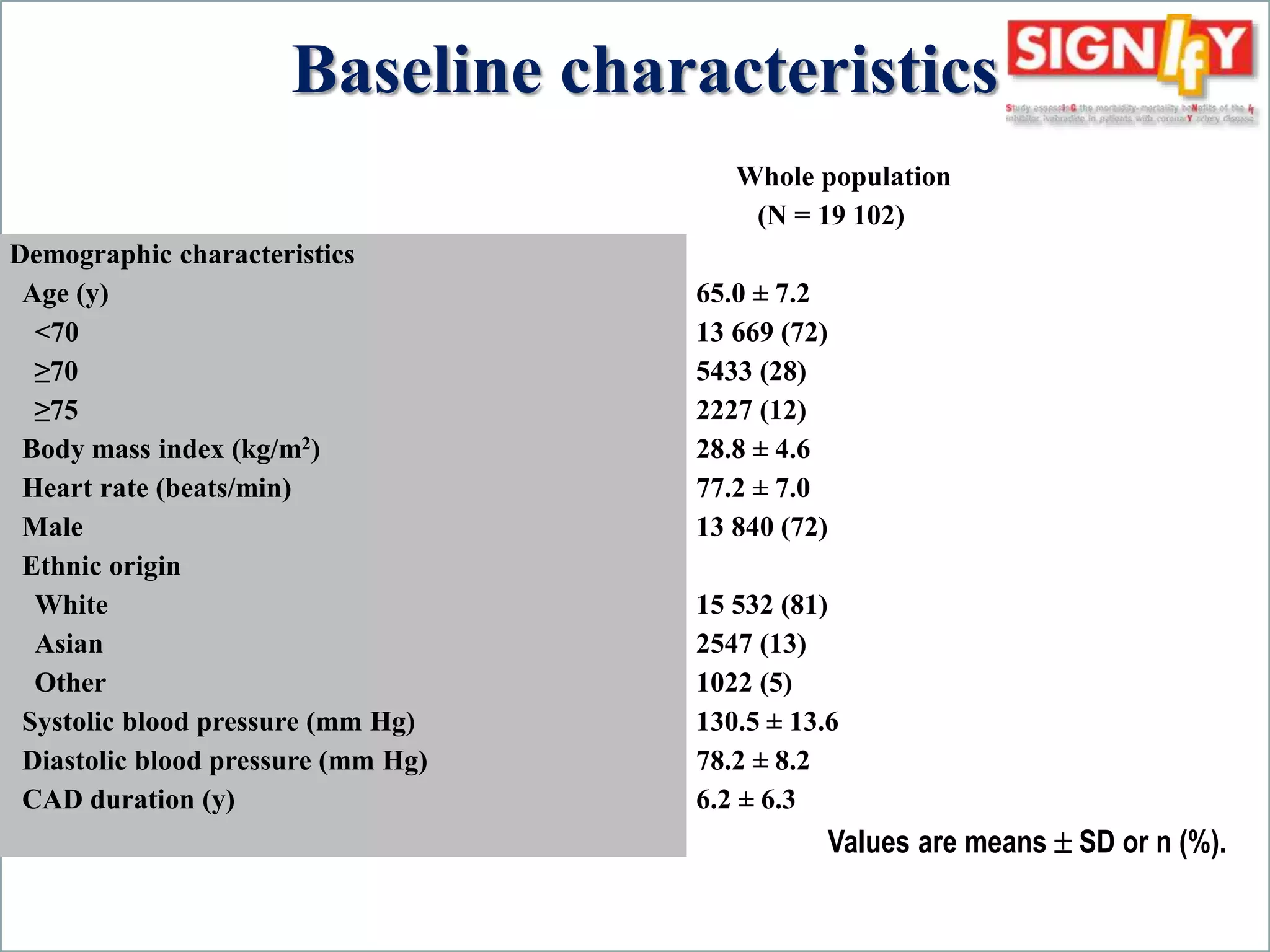
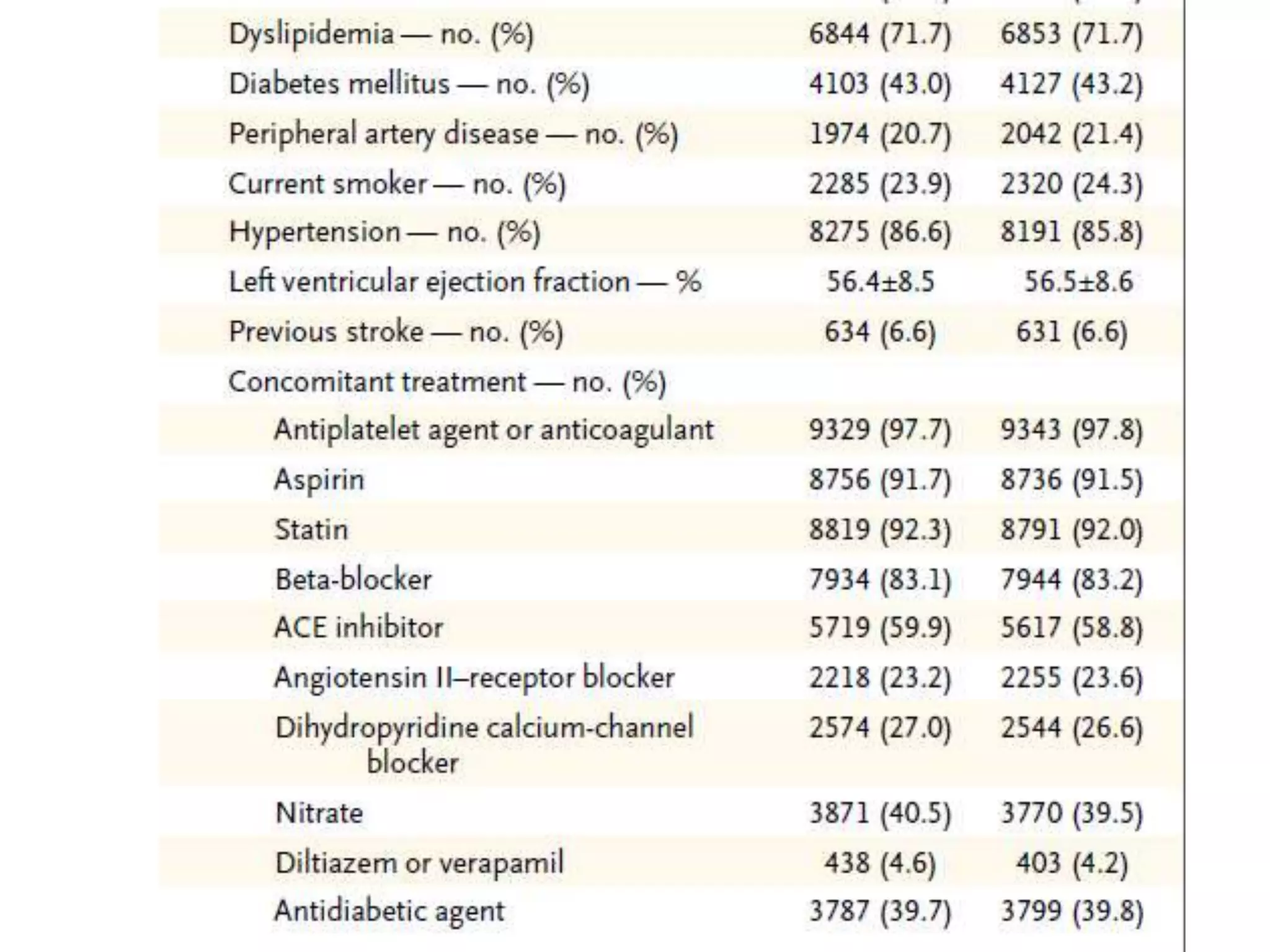
Randomization results showing balanced groups with demographic data including age and heart condition.
Further breakdown of demographics such as age, heart rate, and previous heart incidents.
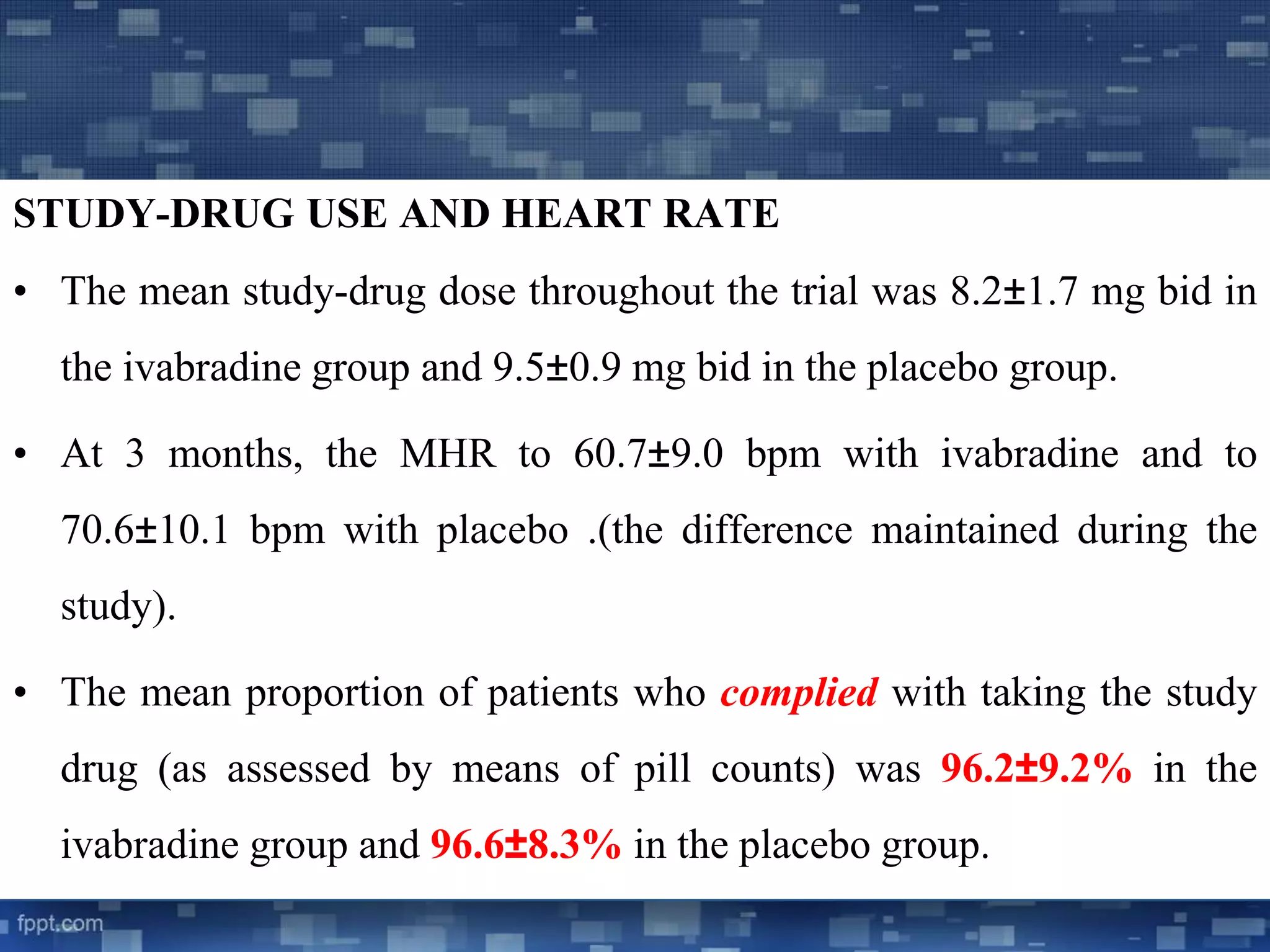
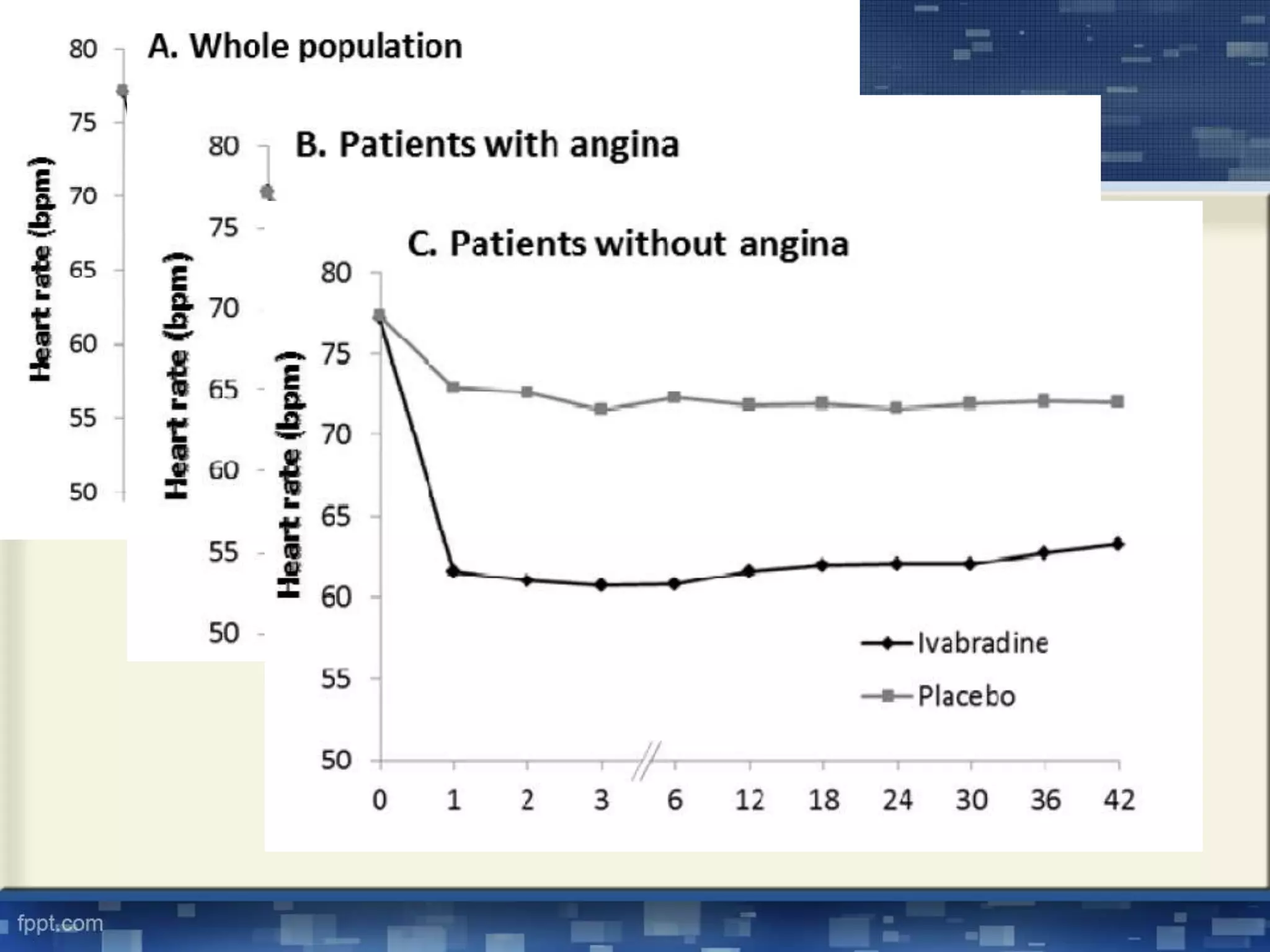
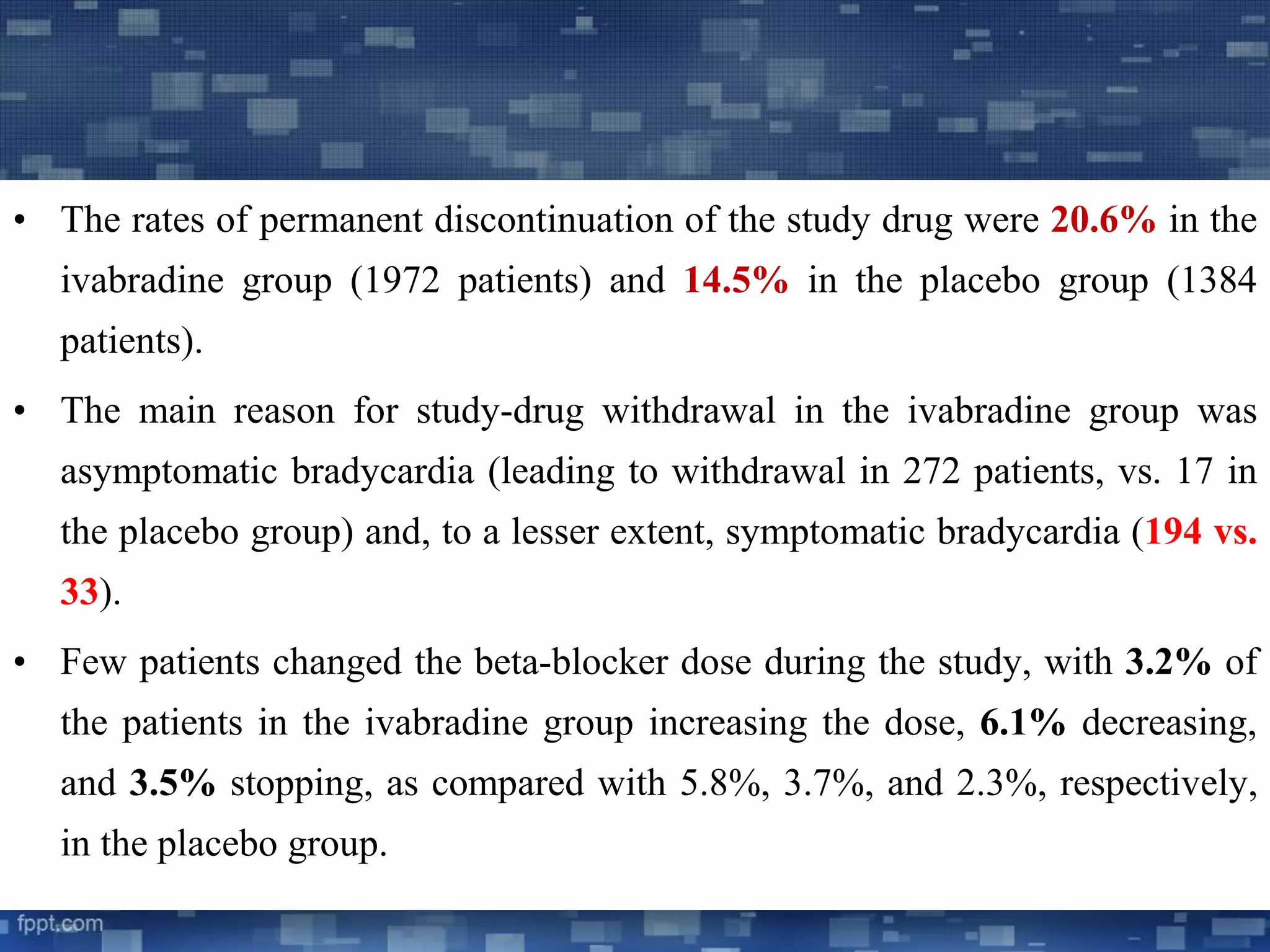
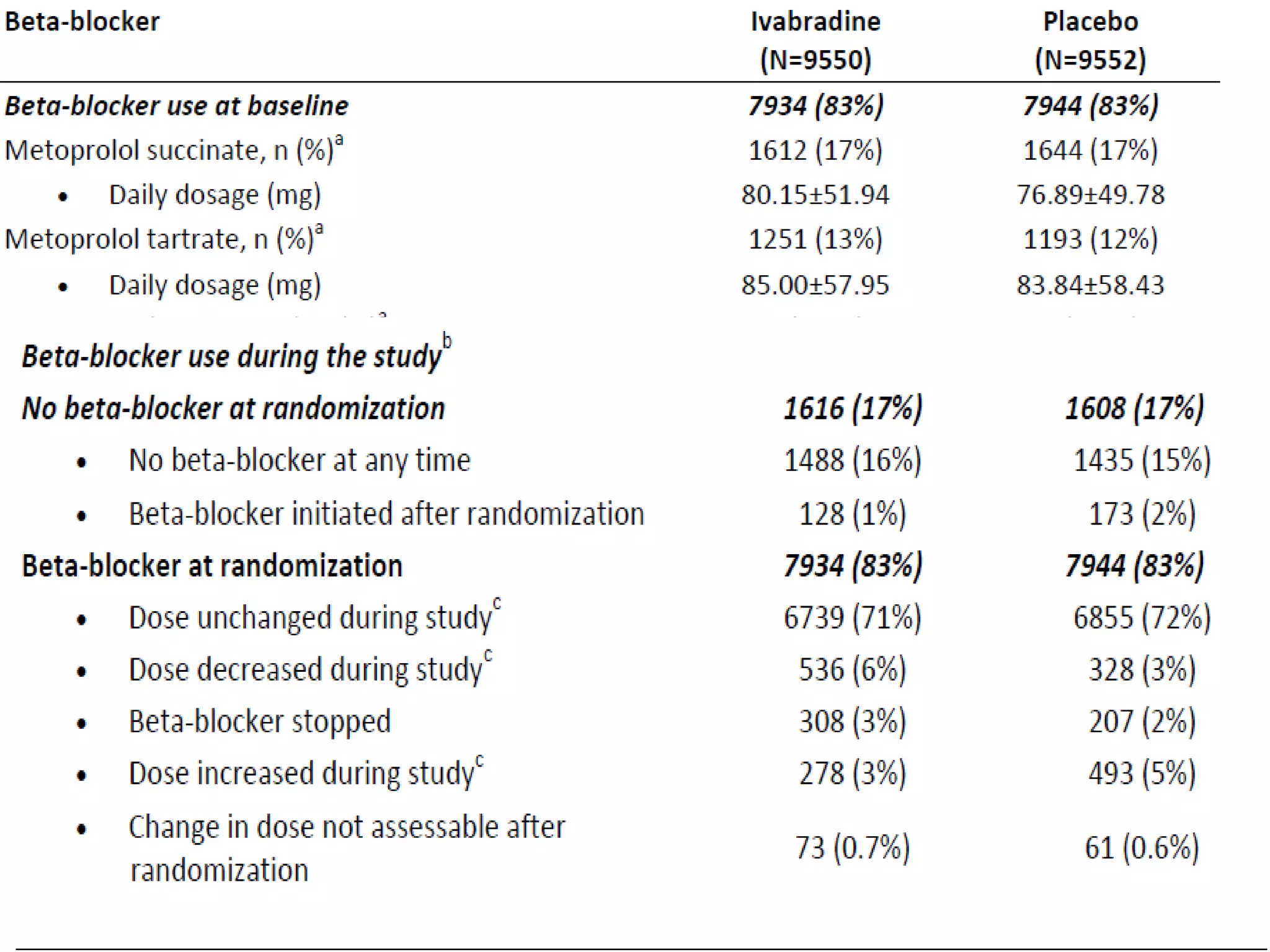
Drug dosage statistics and patient compliance observed throughout the ivabradine trial.
Discontinuation rates due to adverse effects observed in ivabradine vs. placebo groups.
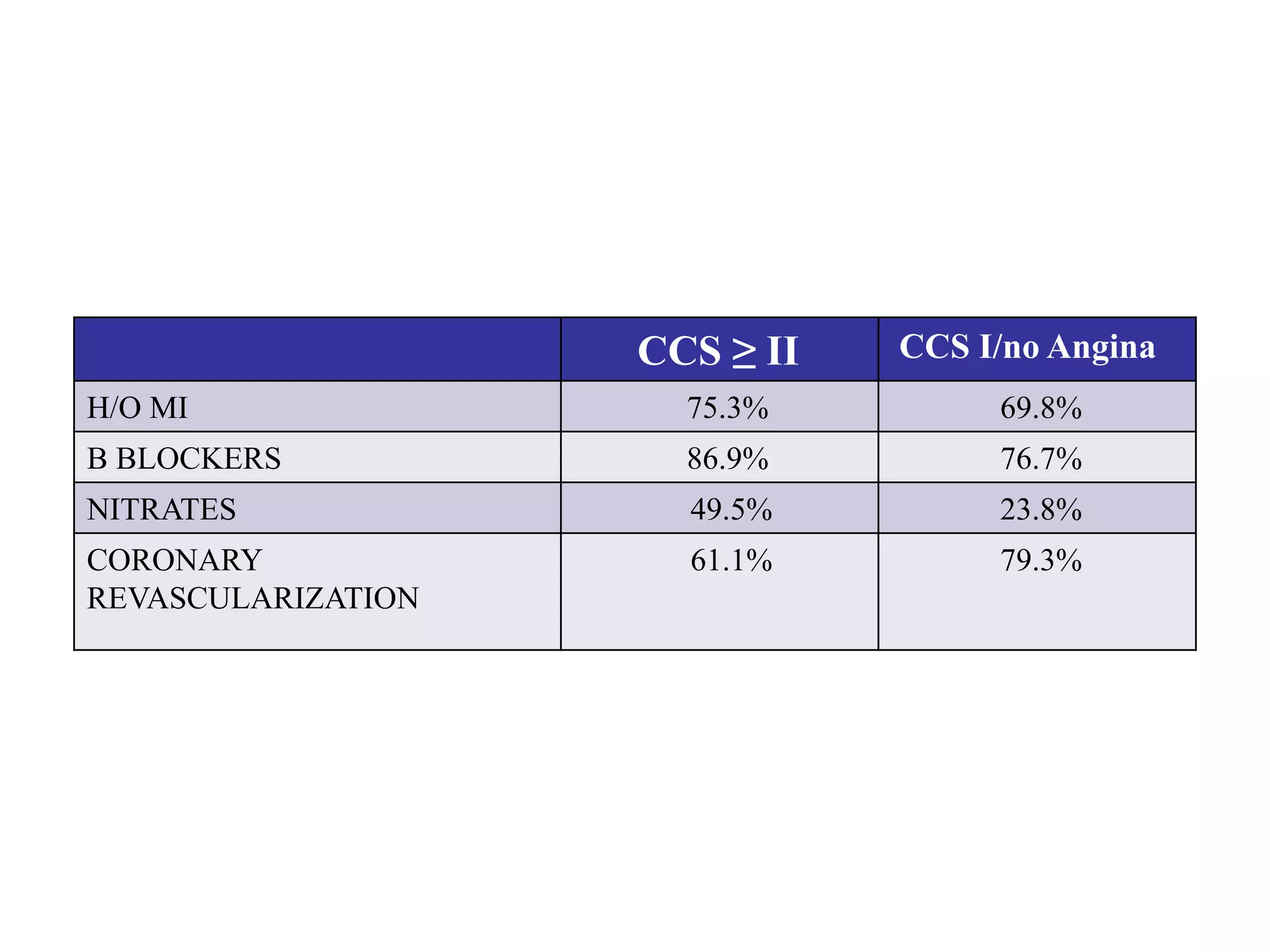
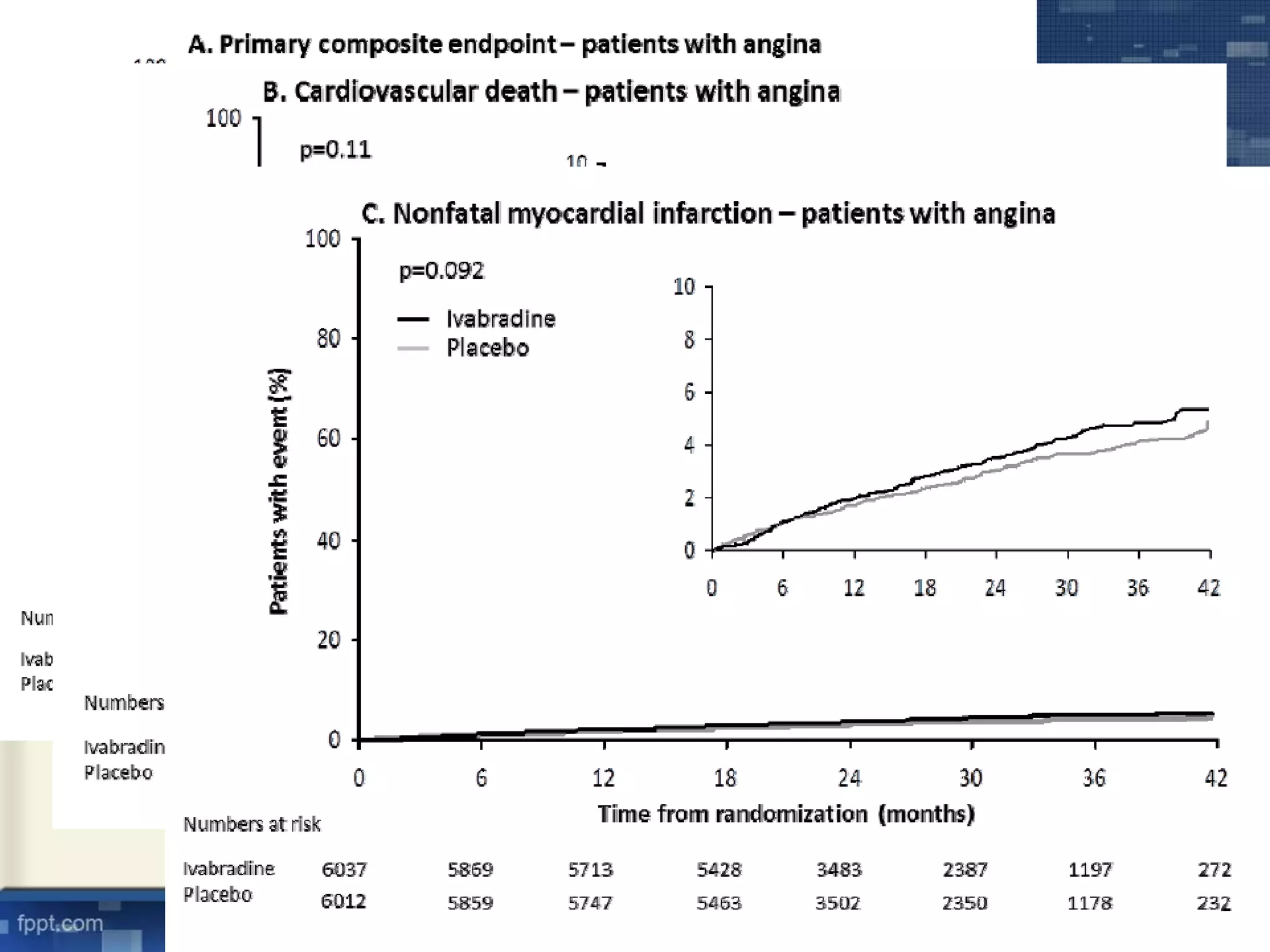
Significant findings among patients, focusing on those with angina and cardiovascular event risks.
Comparison of adverse events reported between ivabradine and placebo groups.
Discussion on the lack of benefit of ivabradine in stable CAD, insights on heart rate's role.
Key conclusions drawn regarding ivabradine's impact on CAD outcomes, emphasizing heart rate's significance.











































































































