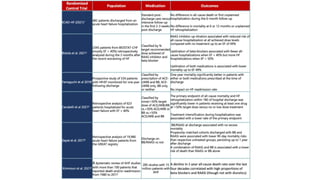
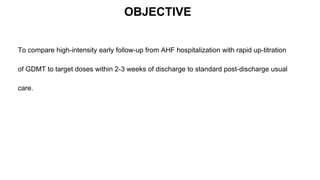
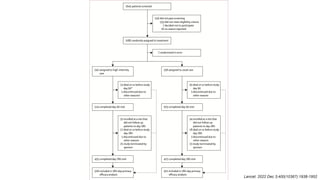
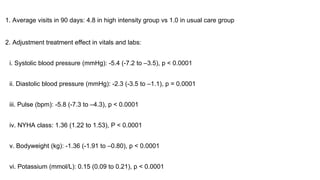
1) The STRONG-HF trial compared a high-intensity follow-up approach focused on rapid up-titration of guideline-directed medical therapies (GDMT) for heart failure to target doses within 90 days of hospital discharge to standard post-discharge care.
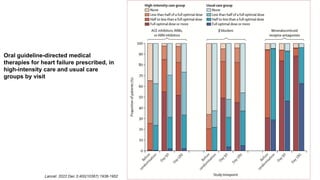
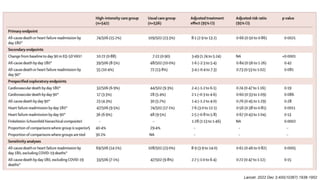
2) The high-intensity approach resulted in significantly higher rates of patients reaching target doses of renin-angiotensin-aldosterone inhibitors, beta-blockers, and mineralocorticoid receptor antagonists by 90 days compared to standard care.
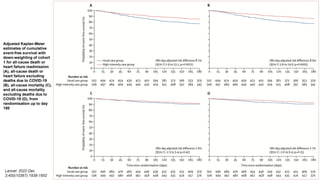
3) At 180 days, the high-intensity approach reduced the combined outcome of all-cause death or heart failure readmission compared to standard care and improved quality of life, with no
























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

















