Downloaded 11 times
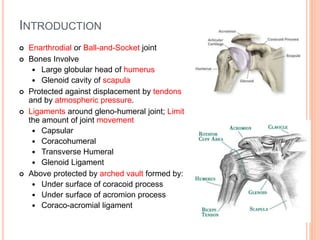
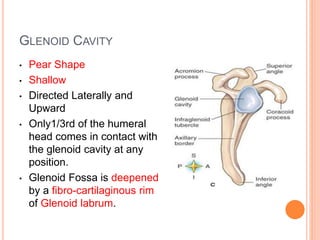
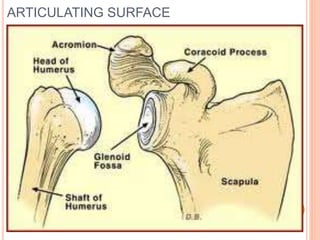
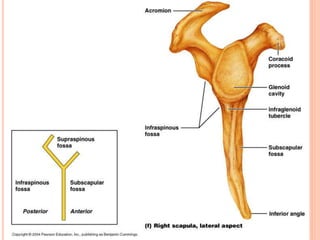

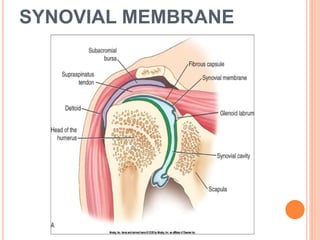
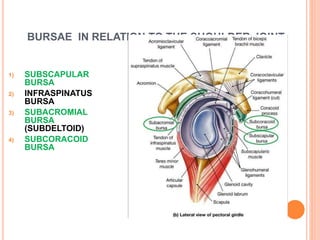
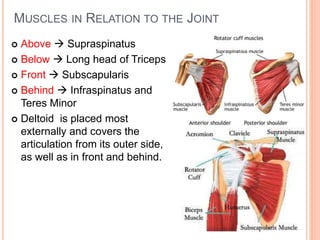
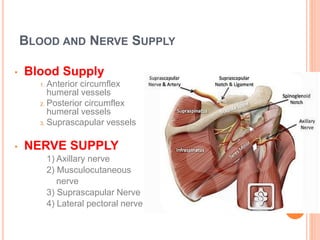
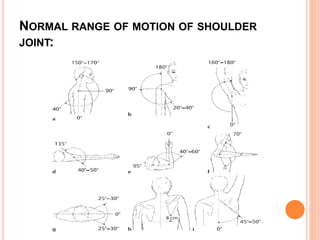
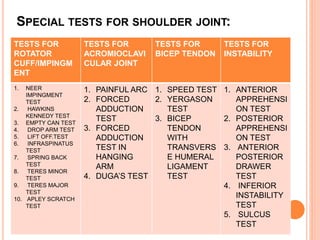
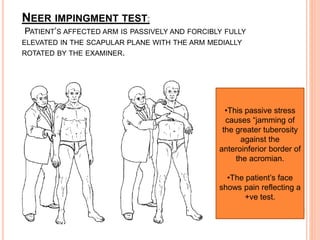
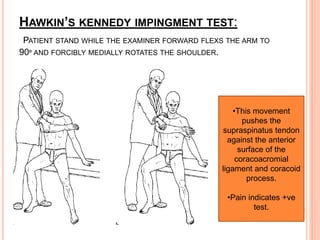






The document provides information on shoulder anatomy and tests. It describes the shoulder joint as a ball-and-socket joint formed by the head of the humerus and glenoid cavity. It details the ligaments, bones, muscles, nerves and vascular supply related to the shoulder. The document also describes various clinical tests used to evaluate the rotator cuff, acromioclavicular joint, biceps tendon and shoulder instability. These include Neer's impingement test, Hawkins-Kennedy test, empty can test and tests for the supraspinatus, infraspinatus, subscapularis and other muscles.





























![Shoulder_joint_and_applied_aspects[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/shoulderjointandappliedaspects1-240425164911-e75cbd49-thumbnail.jpg?width=640&height=640&fit=bounds)





































