1) Shock is a condition where the cardiovascular system fails to adequately perfuse tissues due to impaired cardiac pump function, circulatory issues, or low blood volume.
2) The main types of shock are hypovolemic (low blood volume), cardiogenic (impaired heart function), and distributive (blood vessel problems).
3) Hypovolemic shock results from internal or external fluid loss leading to decreased circulating volume and tissue perfusion. Cardiogenic shock occurs due to impaired left ventricular pumping ability despite normal blood volume.
![Shock SyndromesShock Syndromes
• Hypovolemic Shock
–blood VOLUME problem
• Cardiogenic Shock• Cardiogenic Shock
–blood PUMP problem
• Distributive Shock
[septic;anaphylactic;neurogenic]
–blood VESSEL problem](https://image.slidesharecdn.com/shock-160407203138/85/Shock-for-BS-Medical-technologist-11-320.jpg)
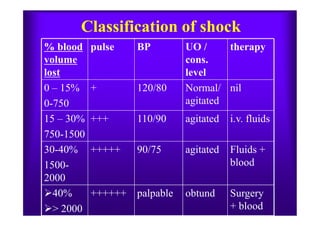
![Assessment & Management
S/S vary depending on severity of fluid loss:
• 15%[750ml]- compensatory mechanism maintains CO
• 15-30% [750-1500ml- Hypoxemia, decreased BP & UOP• 15-30% [750-1500ml- Hypoxemia, decreased BP & UOP
• 30-40% [1500-2000ml] -Impaired compensation &
profound shock along with severe acidosis
• 40-50% - refactory stage:
loss of volume= death](https://image.slidesharecdn.com/shock-160407203138/85/Shock-for-BS-Medical-technologist-17-320.jpg)

![MANAGEMENT OF
NEUROGENIC SHOCK
• Observe for Bradycardia-major
dysrhythmia
• Observe for DVT- venous pooling in
extremities make patients high-risk>>P.E.extremities make patients high-risk>>P.E.
• Use prevention modalities [TEDS,
ROM,Sequential stockings, anticoagulation]
NURSING DIAGNOSIS
• Fluid Volume Deficit r/t relative loss
• Decreased CO r/t sympathetic blockade
• Anxiety r/t biologic, psychologic or social
integrity](https://image.slidesharecdn.com/shock-160407203138/85/Shock-for-BS-Medical-technologist-57-320.jpg)