Downloaded 49 times




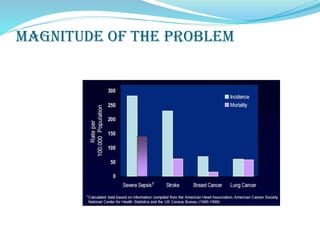


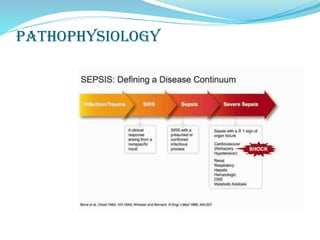









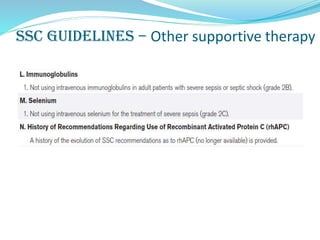



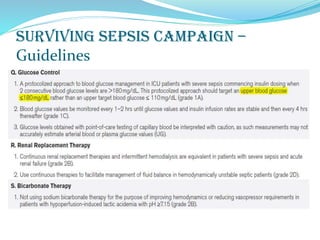
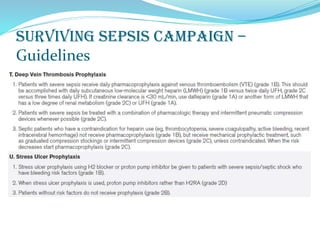
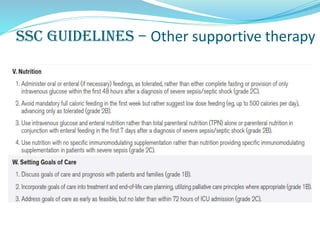








This document discusses sepsis, septicemia, and multiple organ dysfunction syndrome (MODS). It defines related terms like bacteremia, systemic inflammatory response syndrome (SIRS), sepsis, severe sepsis, and septic shock. It discusses the magnitude of the problem globally and in India. It covers the pathophysiology and most common sources of infection. It also summarizes the Surviving Sepsis Campaign guidelines for management of sepsis and septic shock. Finally, it provides an overview of recent advances and controversies in the field and lists various biomarkers that can be used for diagnosis, prognosis, and stratification of sepsis severity.























































































