Downloaded 58 times
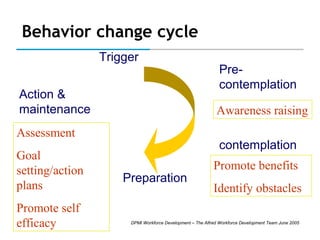



The document provides an overview of promoting behavior change for individuals and populations. It discusses key concepts like the behavior change cycle, self-efficacy, developing resources to support behavior change, tailoring information to stages of change, and self-management principles. Evidence is presented showing self-management education can influence behavior change and improve health outcomes.



































































