Downloaded 14 times

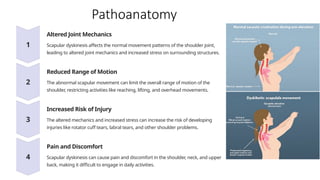
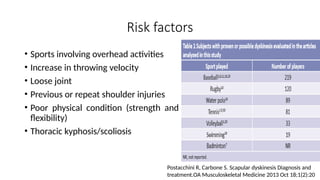
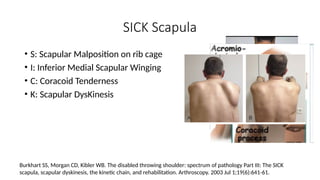
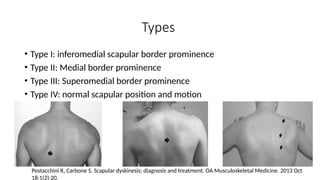
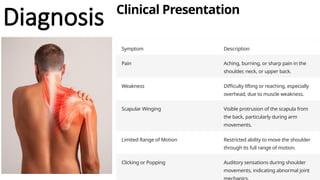
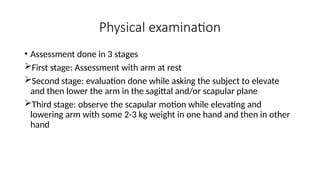
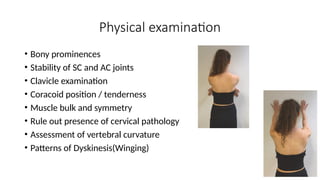
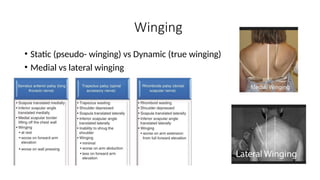


The document discusses scapular dyskinesis, a condition characterized by abnormal scapular motion affecting shoulder function, which can lead to pain and increased risk of injuries. It covers the anatomy of the scapula, biomechanics of shoulder movement, etiology, diagnosis methods, and management strategies including both conservative and surgical approaches. Emphasis is placed on the importance of rehabilitation in restoring optimal scapular motion to prevent further injuries.
















































































