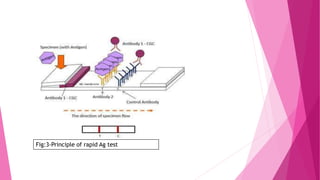
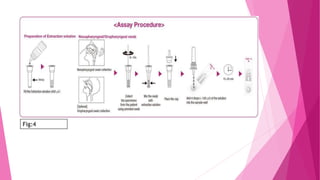
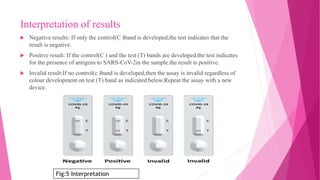


The document outlines the emergence and characteristics of the SARS-CoV-2 virus, which causes COVID-19, and details the rapid antigen test used for its detection. It explains the test's methodology, sample collection, and interpretation of results, emphasizing its importance in diagnosing COVID-19 quickly. Furthermore, it addresses safety precautions, limitations of the test, and references for further reading.






































![RT-PCR by Arnab Kumar Samanta(sen-4^J2020)[133].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/rt-pcrbyarnabkumarsamantasen-4j2020133-221129180252-3c6a6813-thumbnail.jpg?width=640&height=640&fit=bounds)

































