Downloaded 18 times









![Documents to accompany
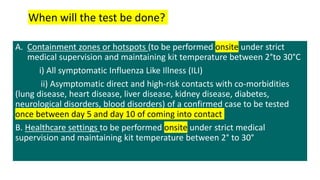
1) Packaging list/proforma Invoice
2) Airway bill (for air transport) (to be prepared by sender or
shipper)
3) Value equivalence document (for road/rail/sea transport)
[ Note: 1. A vaccine-carrier/ice-box can also be used as an outer
container
2. The minimum dimensions of the outer container should
be 10 x 10 x 10 cm (length x width x height)]](https://image.slidesharecdn.com/covid19samplecollectionanddiadnosis-211011011024/85/Covid-19-sample-collection-and-diagnosis-13-320.jpg)

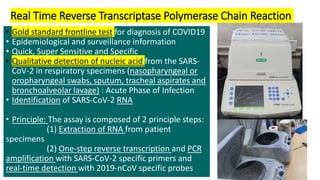

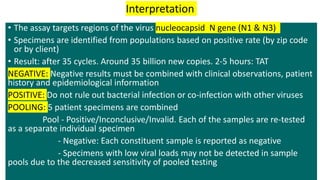



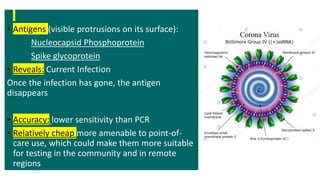





This document provides information on collecting, processing, and diagnosing COVID-19 samples through various methods. It discusses proper sample collection and labeling, as well as packaging and transportation guidelines. The main diagnostic tests described are RT-PCR, which is the gold standard; TRUENAT and CBNAAT, which are chip-based and cartridge-based PCR machines; point-of-care rapid antigen tests; and antibody tests. Precautions for handling specimens and limitations of each test are also outlined.






































![RT-PCR by Arnab Kumar Samanta(sen-4^J2020)[133].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/rt-pcrbyarnabkumarsamantasen-4j2020133-221129180252-3c6a6813-thumbnail.jpg?width=640&height=640&fit=bounds)
























![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)



