
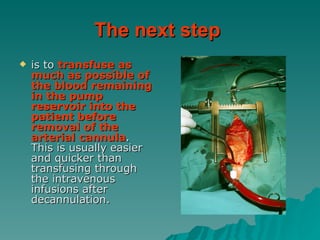
![One approach to weaning from CPB is to bring the filling pressure being monitored (e.g., central venous pressure [CVP], PAOP, LAP) to a specific, predetermined level somewhat lower than may be necessary and then assess the hemdynamics.](https://image.slidesharecdn.com/routinecpbweaning-111207145215-phpapp01/85/Routine-cpb-weaning-12-320.jpg)
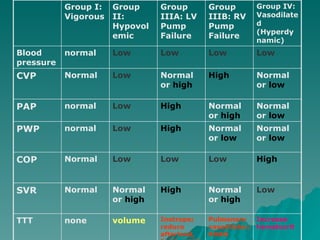



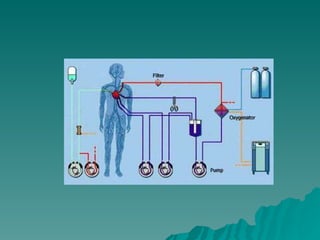
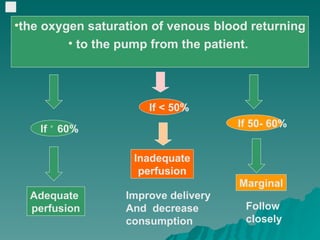
The document outlines the steps for routinely weaning a patient from cardiopulmonary bypass (CPB). It begins with partially occluding venous return to fill the heart and establish pulsatile arterial flow. The perfusionist gradually decreases pump flow while communicating three parameters: flow rate, reservoir volume, and oxygen saturation. As weaning progresses, the patient is assessed for hemodynamic stability before fully clamping venous return and turning off pump flow. Post-bypass, patients are categorized and carefully monitored, with interventions like fluids, drugs or devices as needed to stabilize their condition.



































































![Anaesthesia for cardiopulmonary bypass surgery [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/anaesthesiaforcardiopulmonarybypasssurgeryautosaved-150531185352-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)





























