Download to read offline
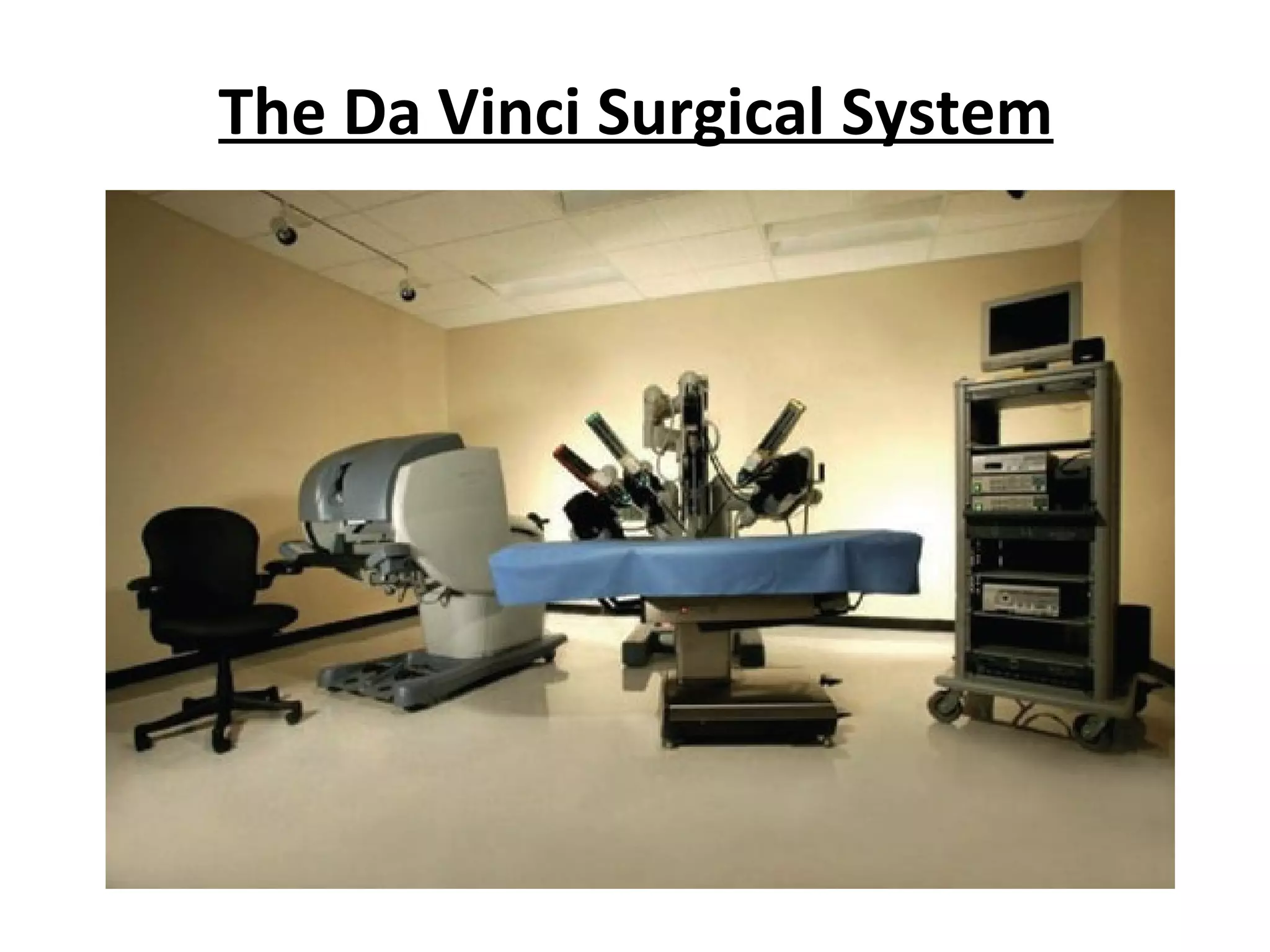
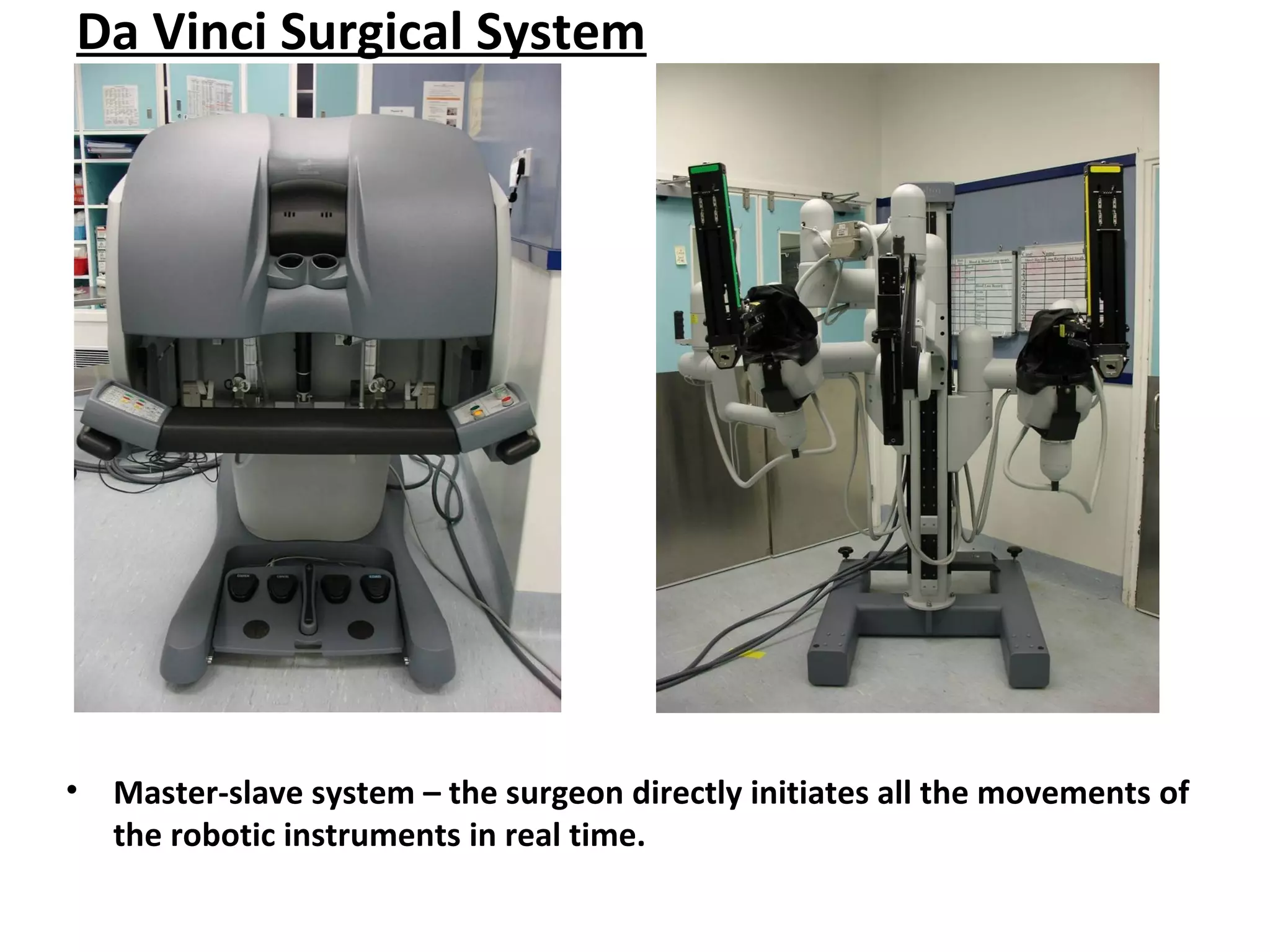
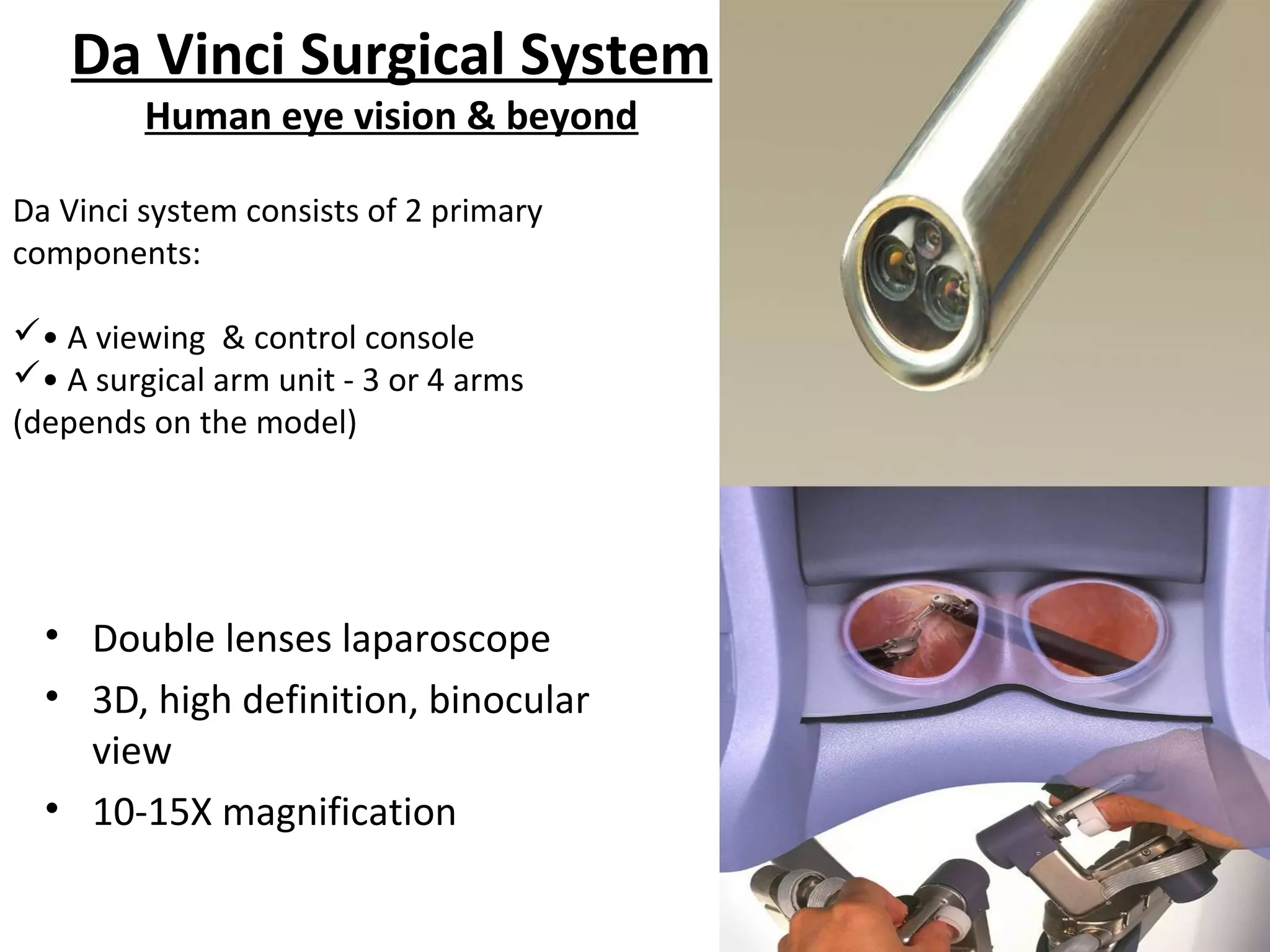
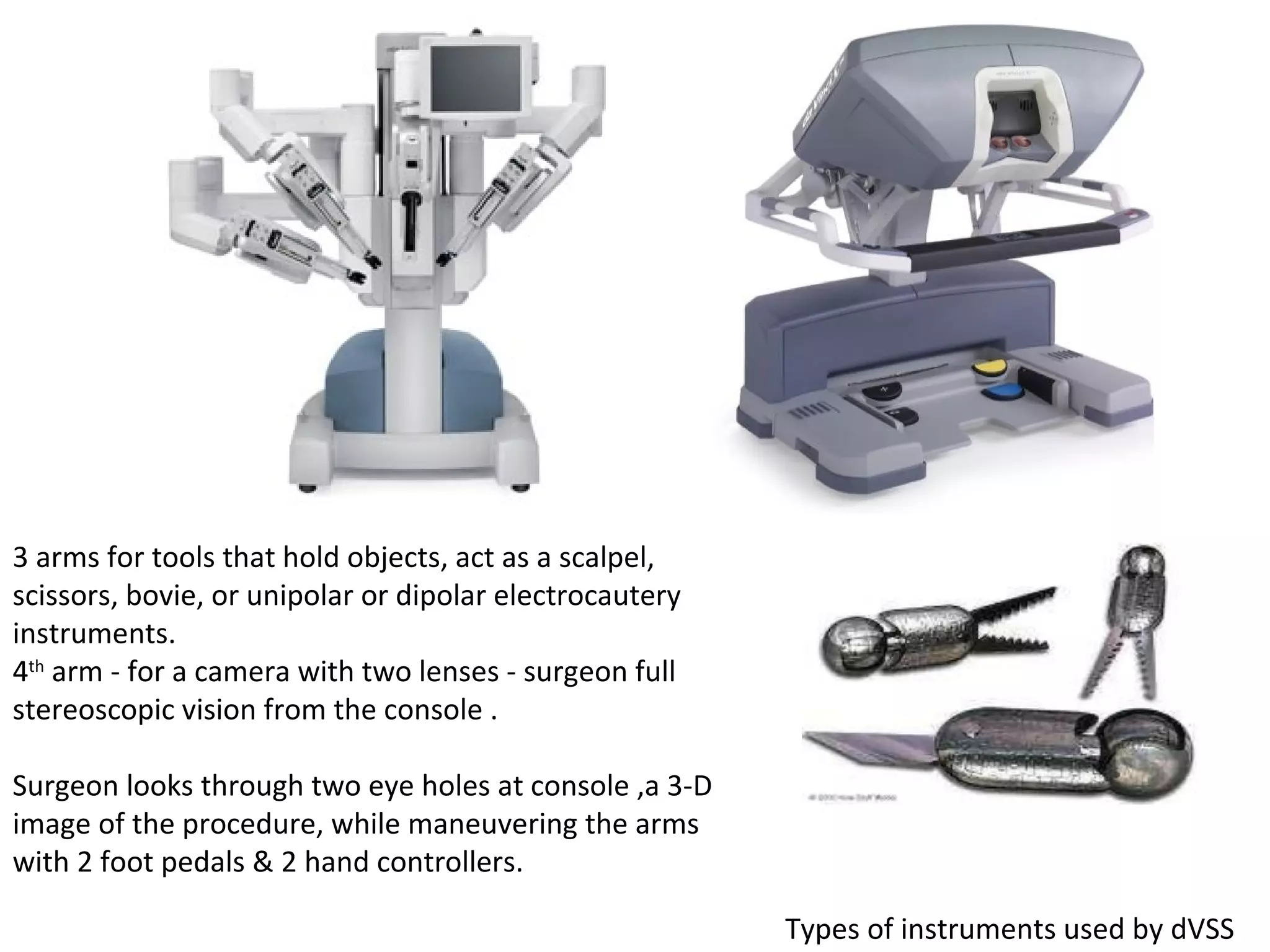


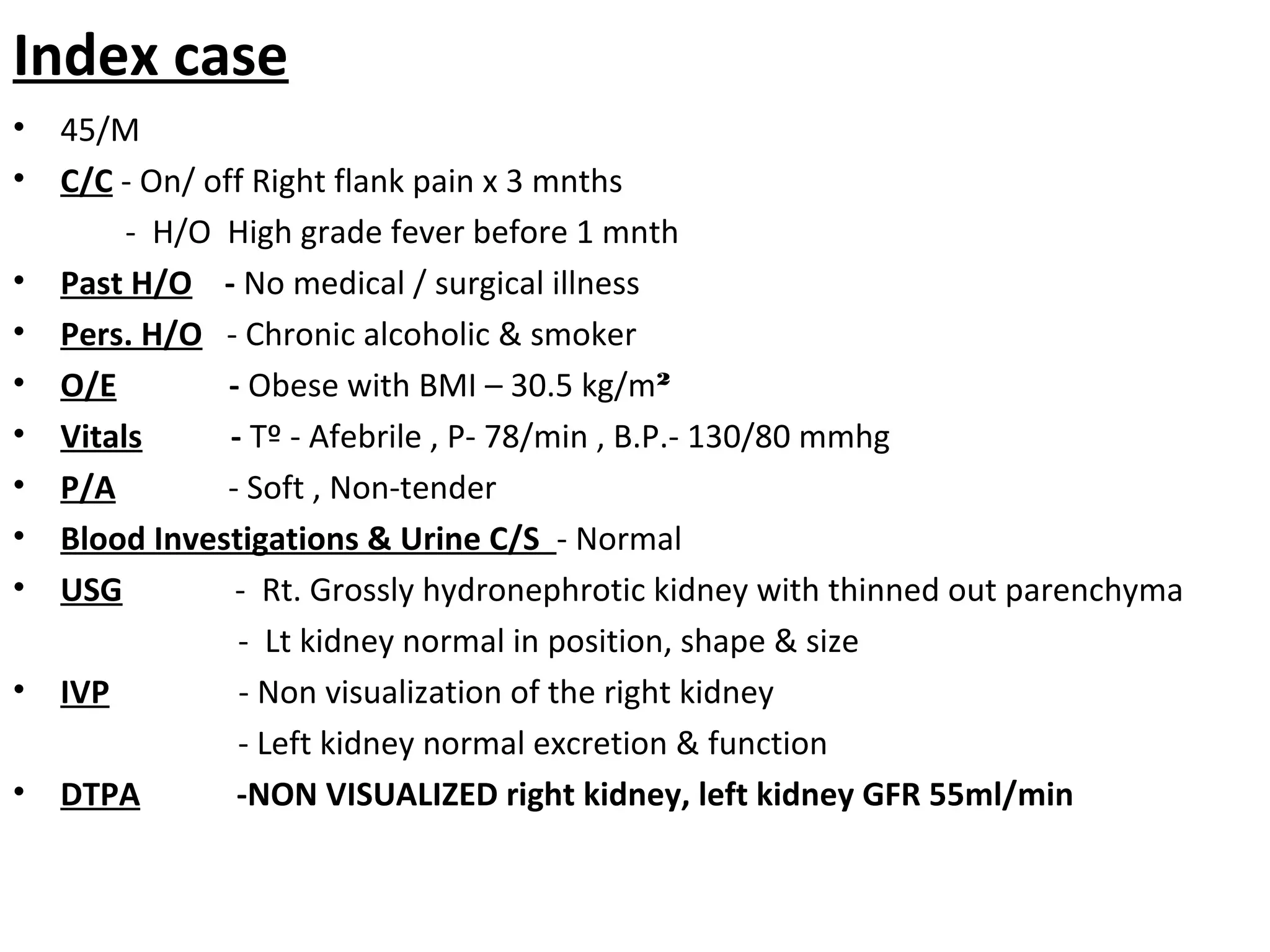
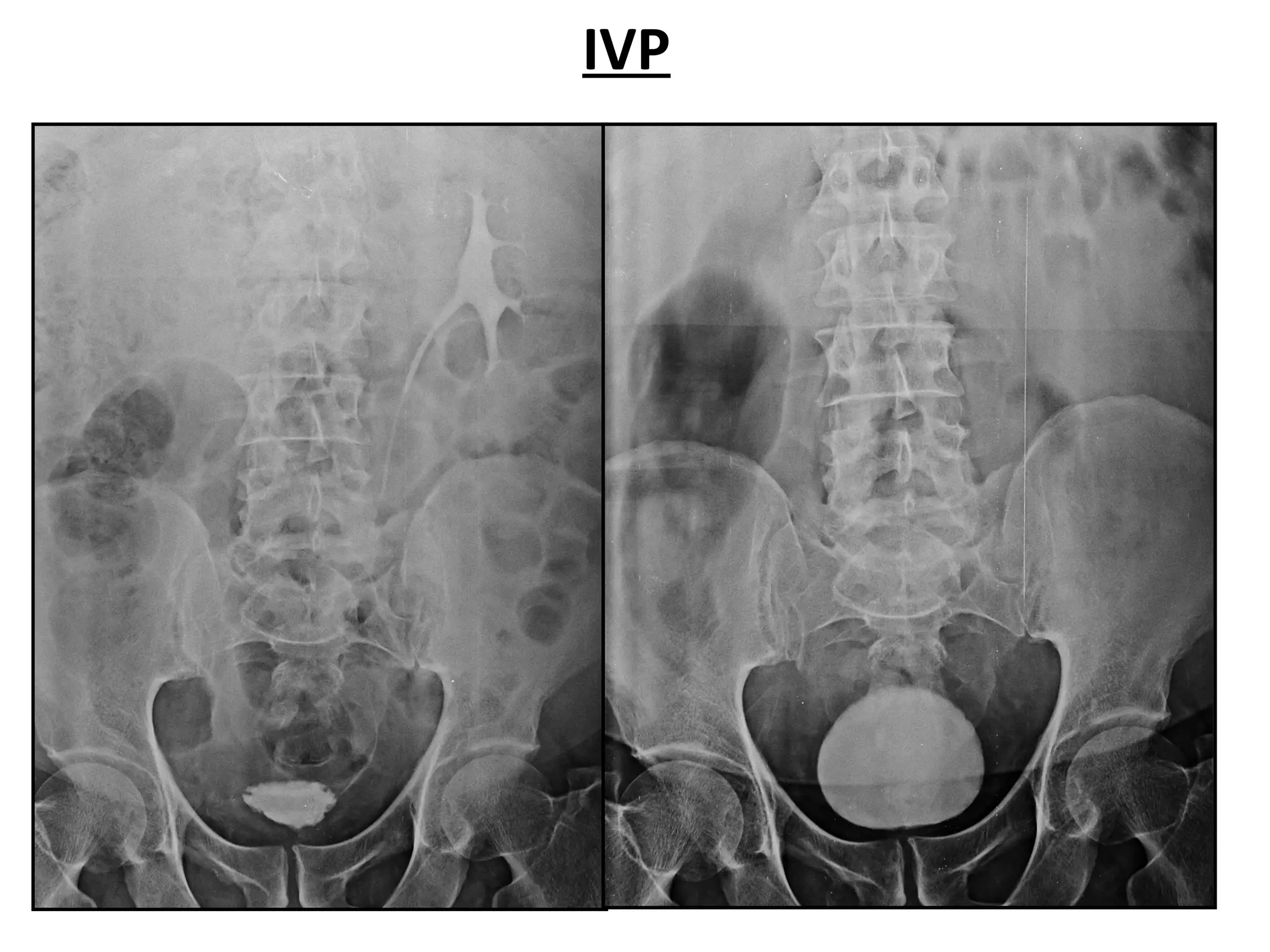
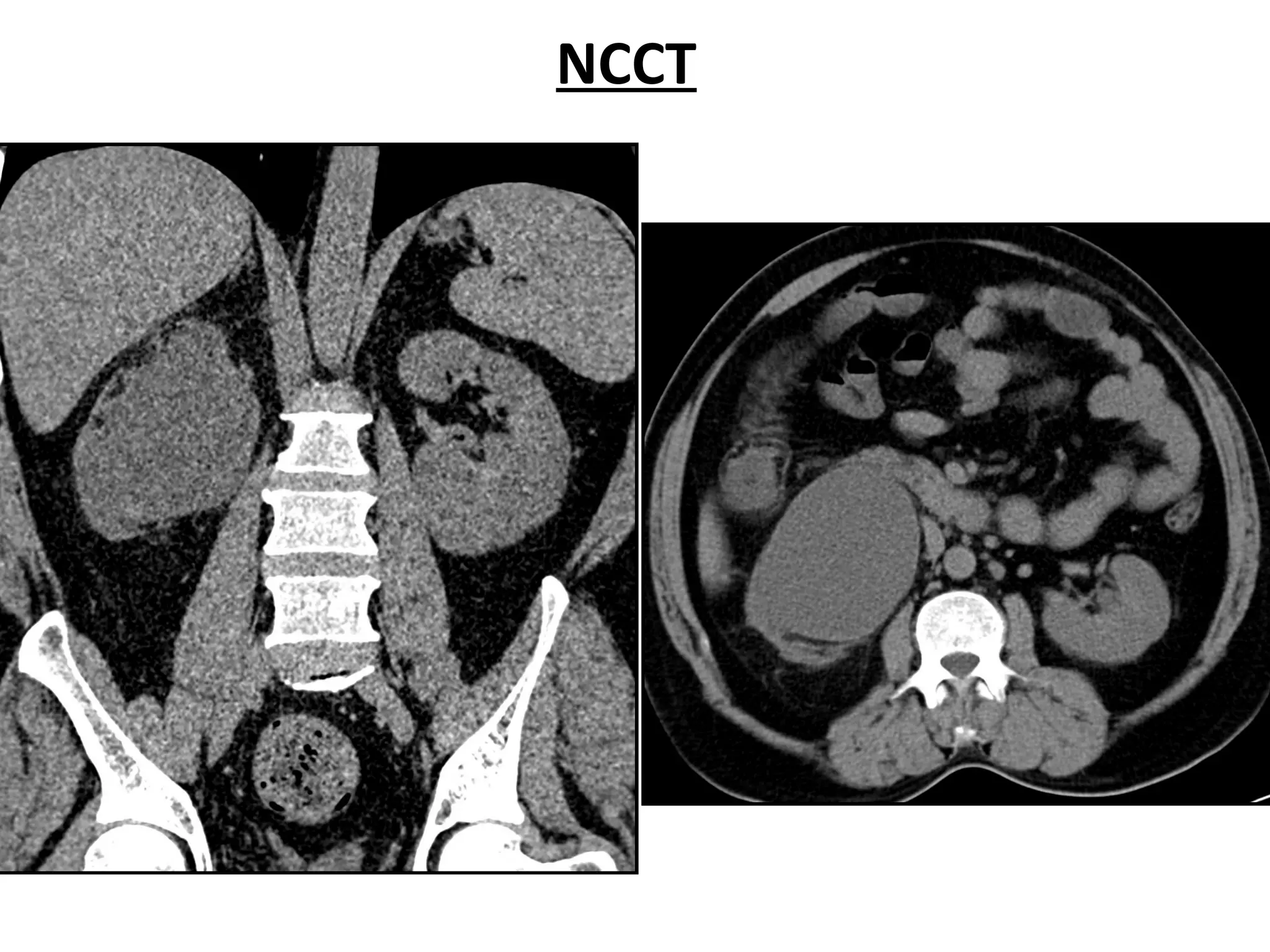
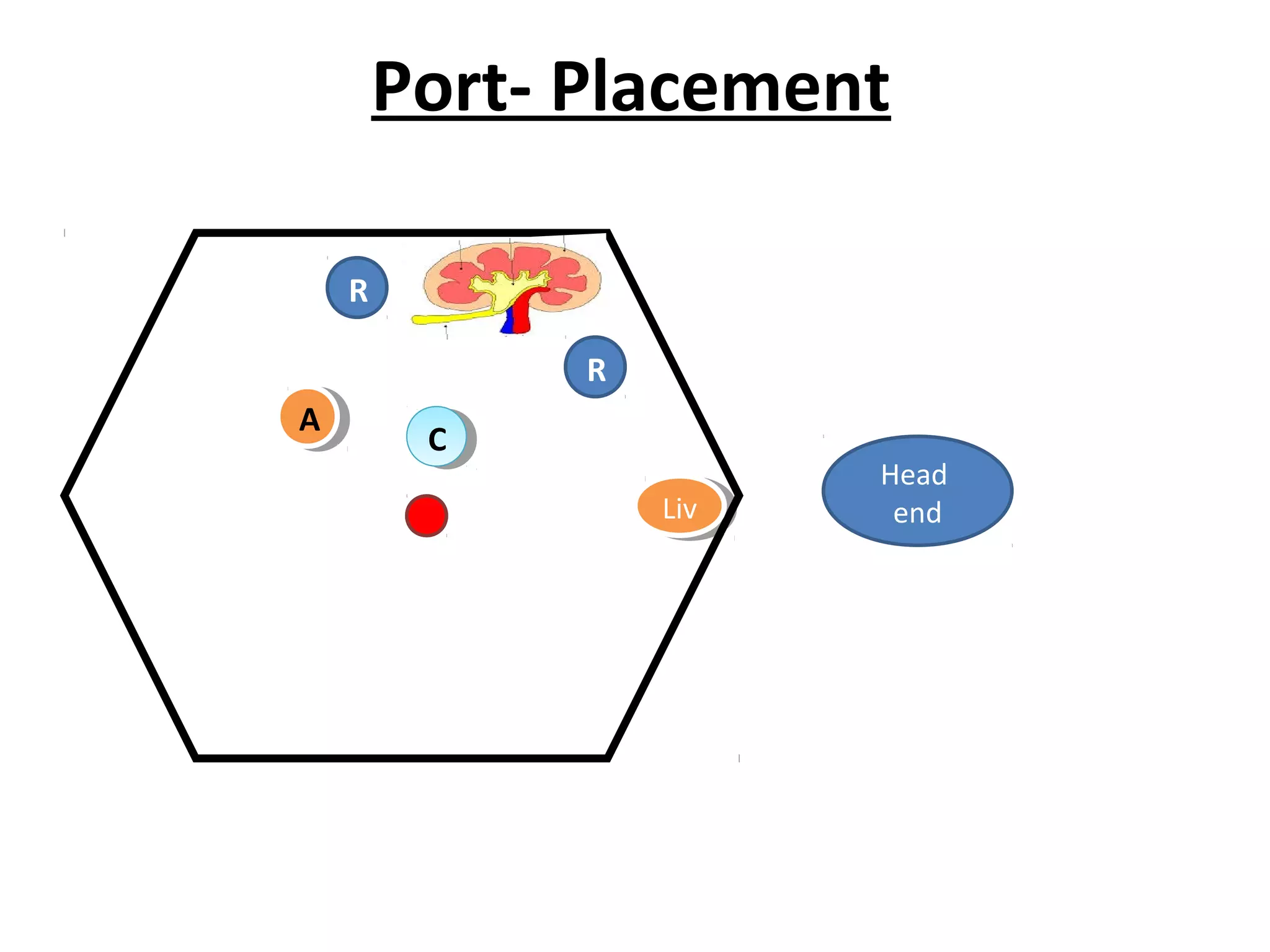


The document discusses robotic assisted laparoscopic nephrectomy using the da Vinci surgical system, highlighting its development, adoption in hospitals, and advanced functionalities. It details the system's components, including a viewing console and surgical arms, and describes a clinical case of right flank pain leading to a nephrectomy. The report concludes with procedural specifics, such as operating time and postoperative outcomes.




![Urinary Diversion after cystectomy [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/urinarydiversionedmond-140716212817-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)













































































