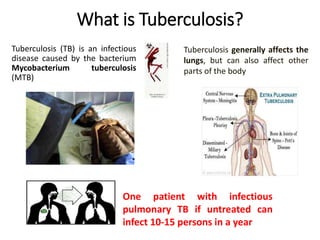
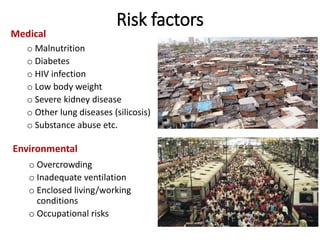
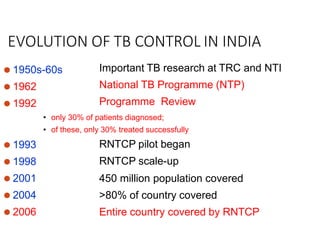
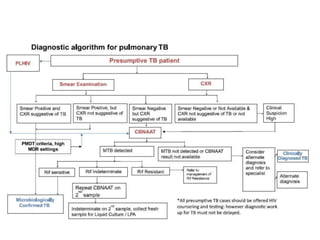
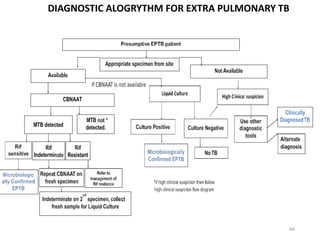
The document summarizes India's Revised National Tuberculosis Control Programme (RNTCP), now called the National Tuberculosis Elimination Programme (NTEP). It discusses tuberculosis (TB) symptoms, risk factors, global and national burden. It describes the evolution of TB control in India from the 1950s to present day. Key aspects of the programme include detecting TB cases through laboratory systems and engaging private sectors, treating all diagnosed TB patients according to drug susceptibility testing results, preventing transmission through airborne infection control and contact tracing, and building health system capacity. The national strategic plan aims to eliminate TB in India by 2025 through goals of detecting, treating, preventing, and building under the NTEP.








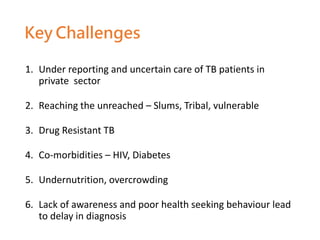






























![National tuberculosis elimination programme [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/nationaltuberculosiseliminationprogrammeautosaved-230623014946-4d00da70-thumbnail.jpg?width=640&height=640&fit=bounds)



































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







