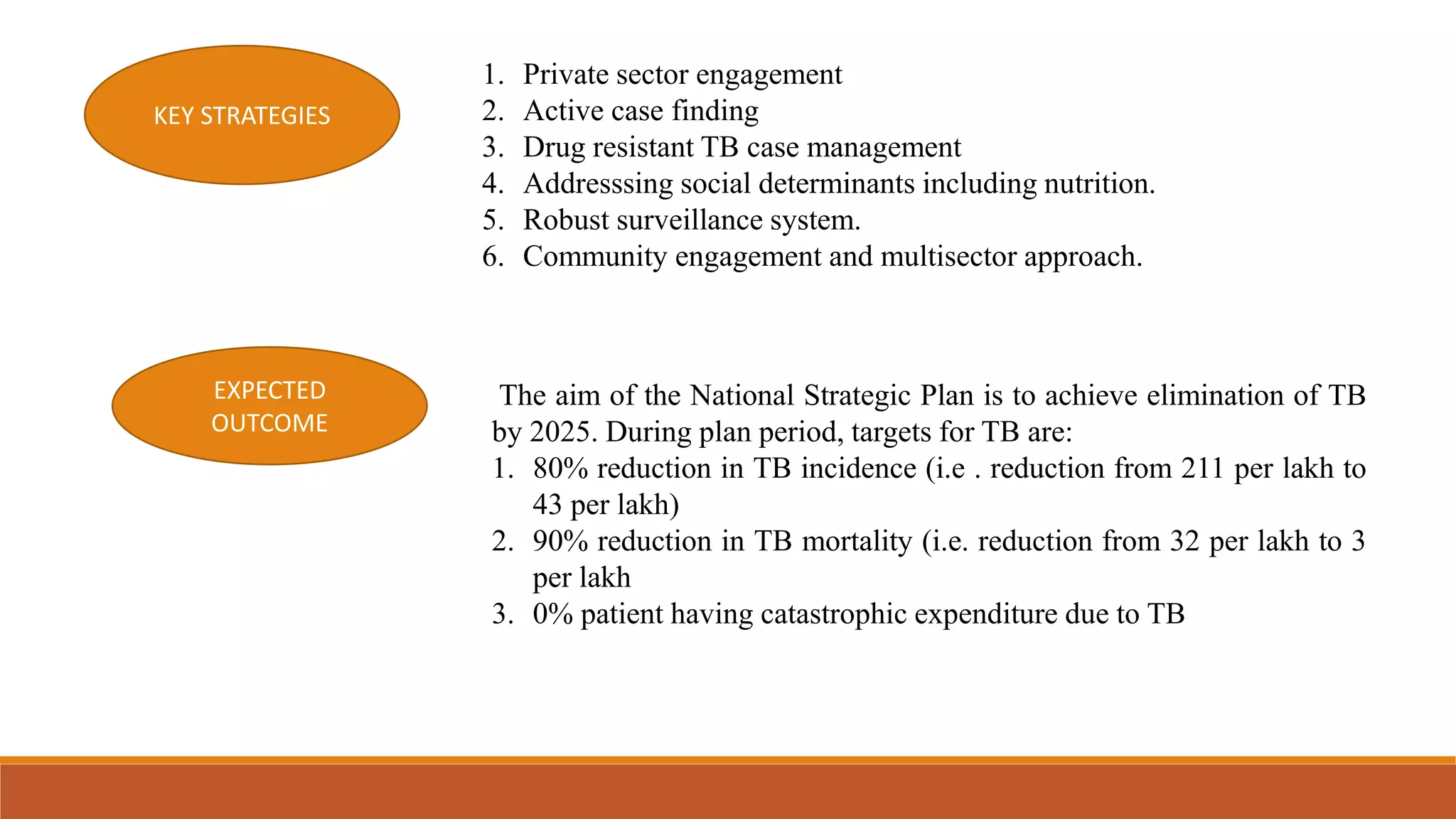
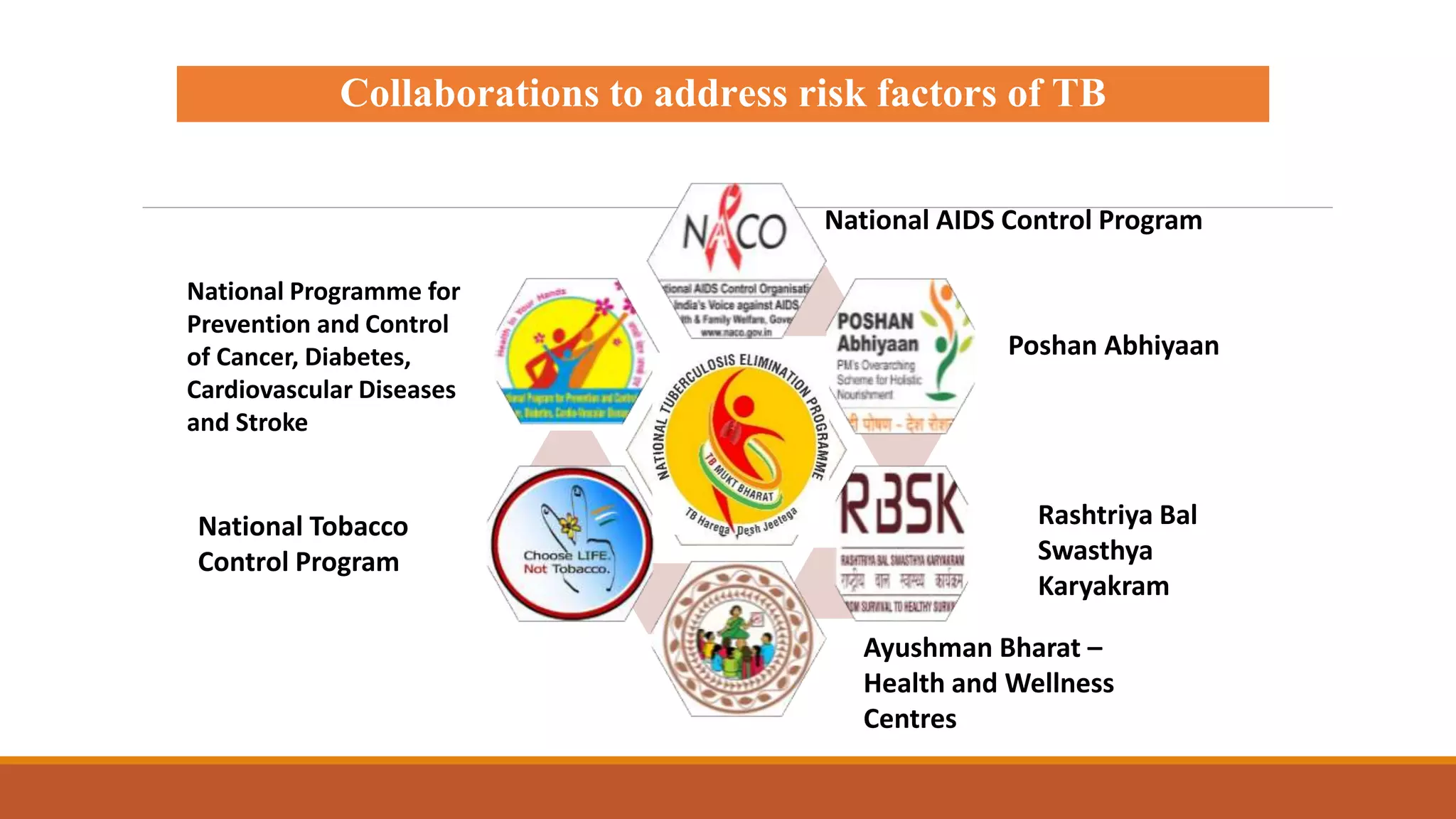
India has moved from a tuberculosis (TB) control program to eliminating TB through its National Strategic Plan for TB Elimination (2017-2025). Key challenges include engaging private providers, addressing drug-resistant TB, and preventing new TB cases. The plan aims to reduce TB incidence and mortality by 80% and 90% respectively by 2025. Strategies include engaging private providers, active case finding, addressing social determinants, and a multisectoral approach. The government's digital Nikshay program tracks TB cases and outcomes nationwide to support elimination goals.



























![National tuberculosis elimination programme [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/nationaltuberculosiseliminationprogrammeautosaved-230623014946-4d00da70-thumbnail.jpg?width=640&height=640&fit=bounds)































































