1
FEDERAL TEACHING HOSPITALKATSINA.
DEPARTMENT OF OBSTETRICS AND
GYNAECOLOGY.
Procedural Presentation On
MANAGEMENT OF RETAINED PLACENTA
By
Dr Nafisa Abubakar Haruna {Registrar}
Supervised by
Dr Shehu Jamiu {Senior Registrar}
8th
/02/ 2024
3
Introduction
Retained placentais a recognized cause of
primary post partum haemorrhage
associated with increased risk of maternal
morbidity and mortality
Incidence is based on the time chosen, in
90% placenta delivers within 15mins, in 96%
within 30mins and within 60mins in 98%.
Delivery timing of placenta depends on the
type of management .
Treatment can be medical or surgical
4.
4
definition
Retained placenta:Failure to deliver
the placenta within 30mins after
delivery of the fetus.
There is a 10 fold increased in the risk
of hemorrhage and the chance of
spontaneous delivery of the placenta
decreases if the third stage exceed
30mins.
5.
5
Types & riskfactors
Trapped placenta Placenta adherence Placenta accreta
Premature
contraction of lower
uterine segment
Preterm labour preeclampsia
Iv ergometrine Uterine fibroids miscarriage
Full bladder Induction of labour Uterine anomaly
Oxytocin
augmentation
Uterine scar
8
Manual removal of
placenta
Is one of the treatment modalities , a
life saving procedure associated with
maternal morbidity and mortality if
not done carefully.
Should be done by trained health
care provider in the operating room
under anaesthesia.
9.
9
Manual removal placenta
Pre-procedure:
Counsel
Consent
Investigations
Book theatre and inform anesthetist
Empty urinary bladder
Pre -induction broad spectrum
antibiotics
10.
10
procedure
Transfer thepatient to theatre
Provide general anaesthesia that relaxes the
uterus
Place patient in lithotomy position
Surgeons scrub and gown
Clean and drape patient
Attempt controlled cord traction
Hold umbilical cord with the left hand and
insert the right hand {cone shaped} into the
vagina, trace the placenta along the cord to its
insertion in the uterus
11.
11
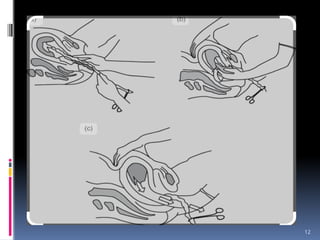
Cont….
Gently usethe cone shaped hand to dilate
the cervix incase its partially closed
Drop the umbilical cord on the left hand
and move the hand to the anterior
abdominal wall to grasp and stabilize the
uterine fundus
Located the cleavage plane between the
placenta and the uterus with the ulnar
border of the right hand
With a see-saw movement ,gradually shell
the placenta from the uterus
13
Cont…
Hold theplacenta in the cupped right hand and
provide counter traction on the uterus using the
hand on the anterior abdominal wall while
withdrawing the right hand holding the placenta
from the uterus
After complete removal , hand over the placenta to
assistant to examine for completeness
Ovum forceps maybe used to explore the uterus
if there is any missing cotyledon or part of the
membranes.
Examine patient for genital tract tear and repair
Clean patient, reposition and revert anaesthesia
14.
14
Post -procedure
Administer10 i.u oxytocin IV
Set up high dose oxytocin infusion
over 4-6hrs
Parenteral antibiotics and IVF for 24-
48hrs
Transfuse appropriately
Monitor for vital signs closely
Monitor for vaginal bleeding
Debrief the woman.
15.
15
complications
Early late
Post partumHemorrhage Uterine synechia
Uterine perforation Secondary infertility
Infection Chronic pelvic pain
Uterine Inversion
16.
16
conclusion
Active managementof third stage of
labour can prevent and reduce the
incidence of retained placenta
Manual removal of placenta is a life
saving procedure that must be
known by all trainees
17.
17
Reference
Paterson-brown S.Obstetrics emergencies In: Edmond D, K(ed) dewhurst
textbook of Obstetrics and Gynaecology. 9th
edition Oxford: John Wiley &
Sons Ltd; 2018. 336-353.
Weeks AD. Retained placenta. In:Thomas FB,Andrew A.C,Sabaratnam A
(eds.) Munro Kerr’s Operative Obstetrics, 12th
ed.London :Saunders
Elsevier Ltd ;2014:207-10.
Konar H.DC Dutta’s Textbook of obstetrics 7th
ed.New Delhi : Jaypee
Brothers Medical Publishers LTD; 2013:p418-9
Andrew DW. The Retained Placenta. Best practice & Research Clinical
Obstetrics and Gynaecology 2008;22(6); 1103-1117
Lo Lawani , Basic steps in obstetrics and gynaecological procedures 2nd
edition 2021: 244-247