Downloaded 82 times


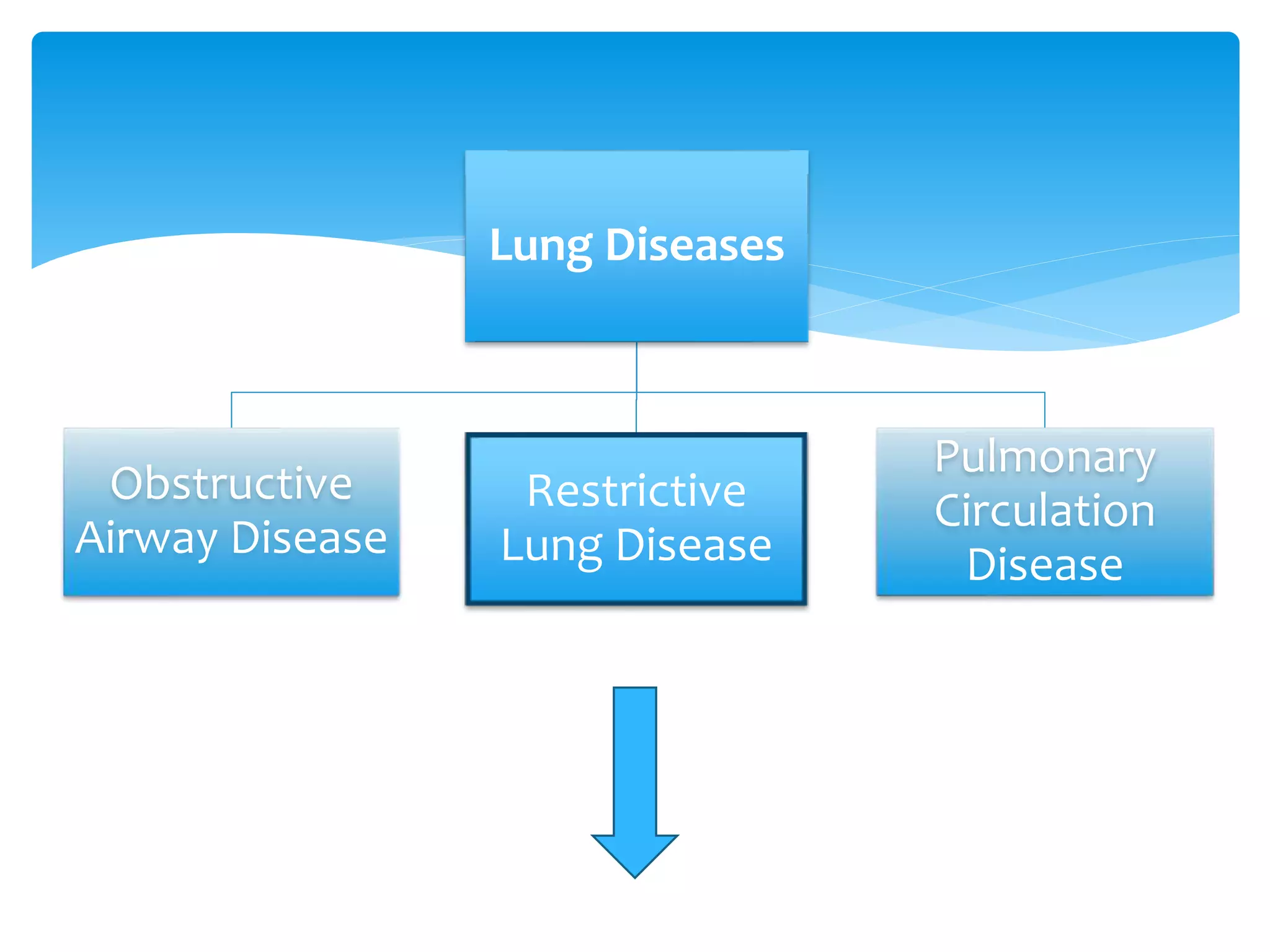







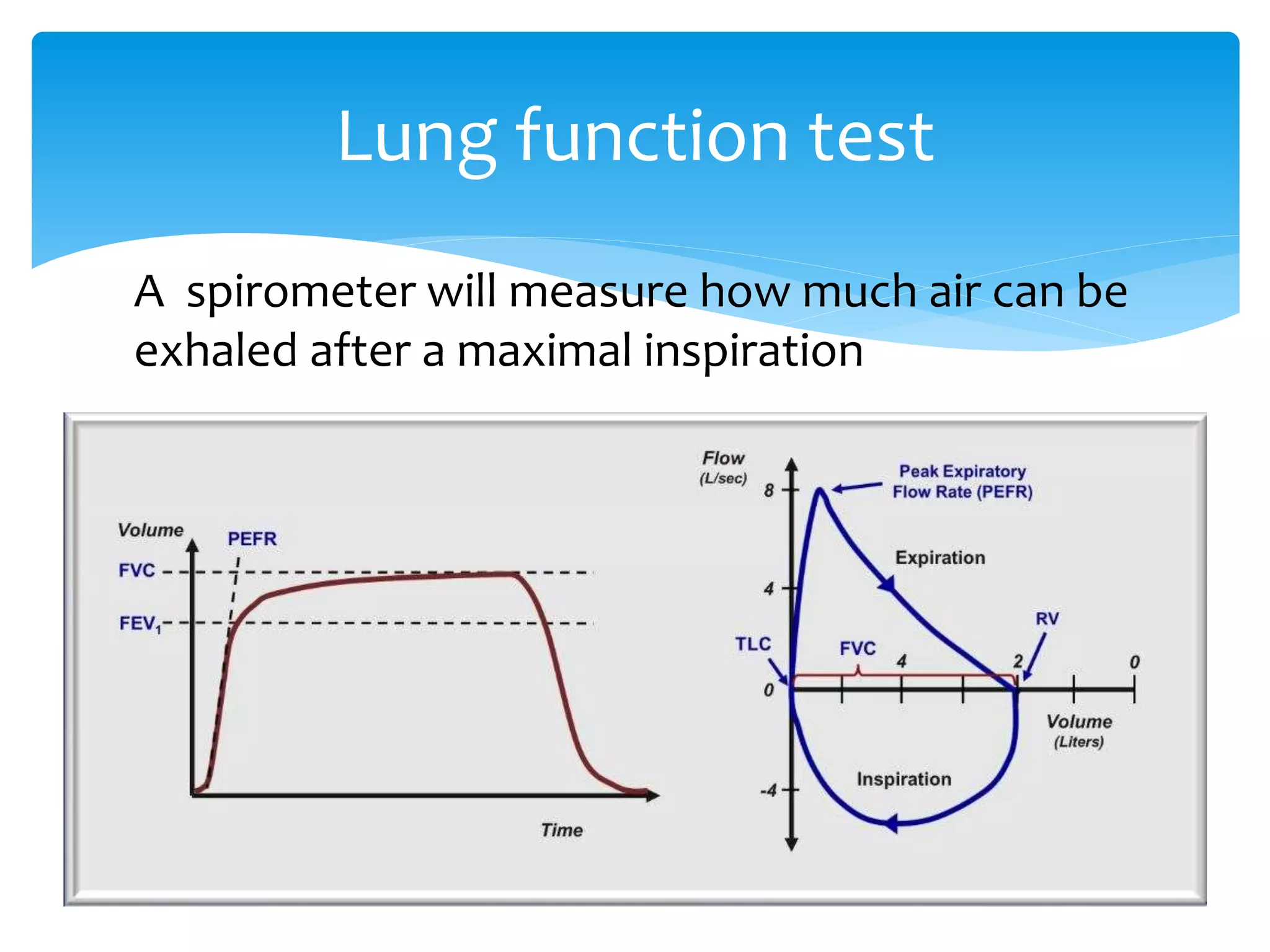

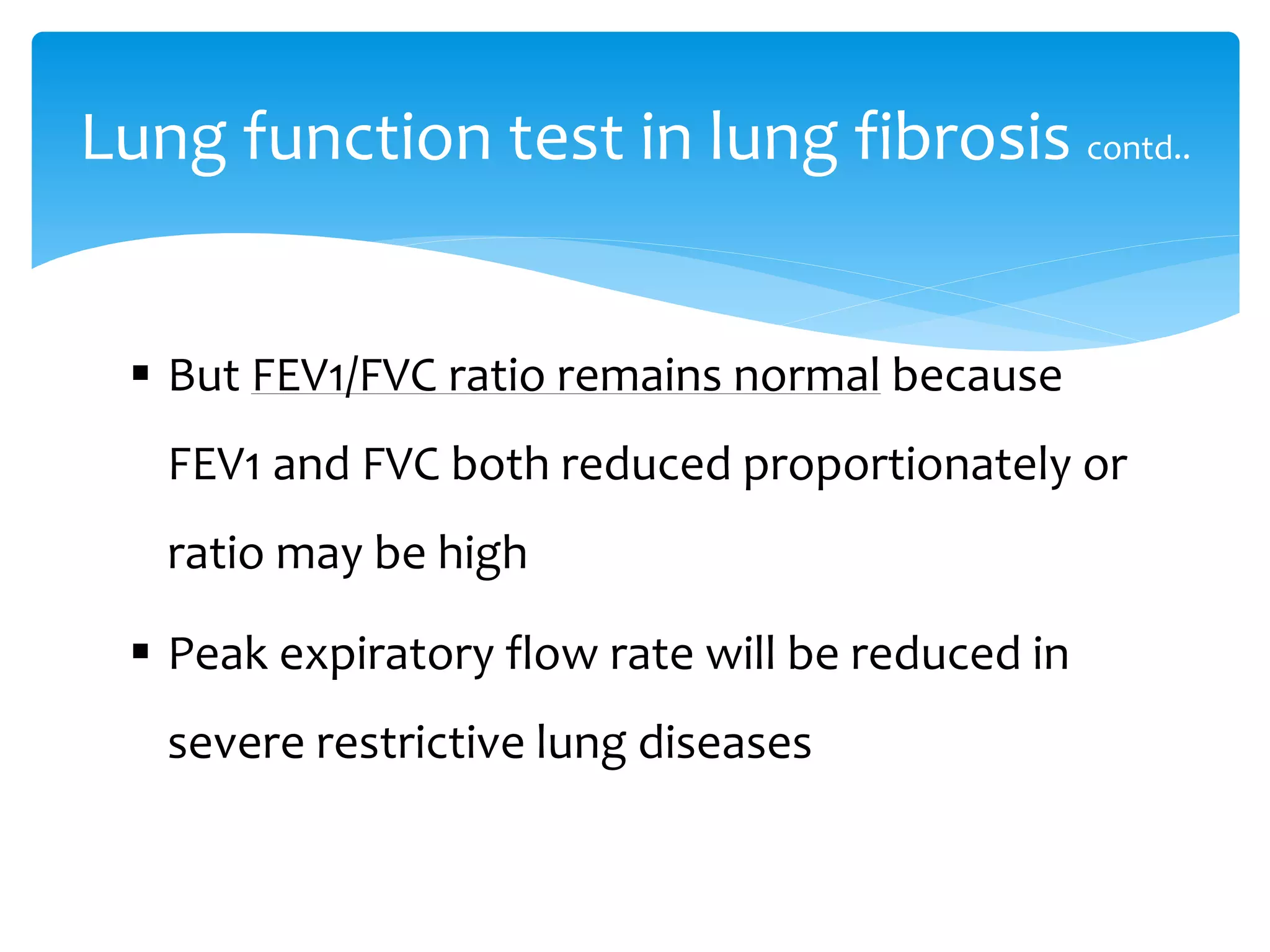

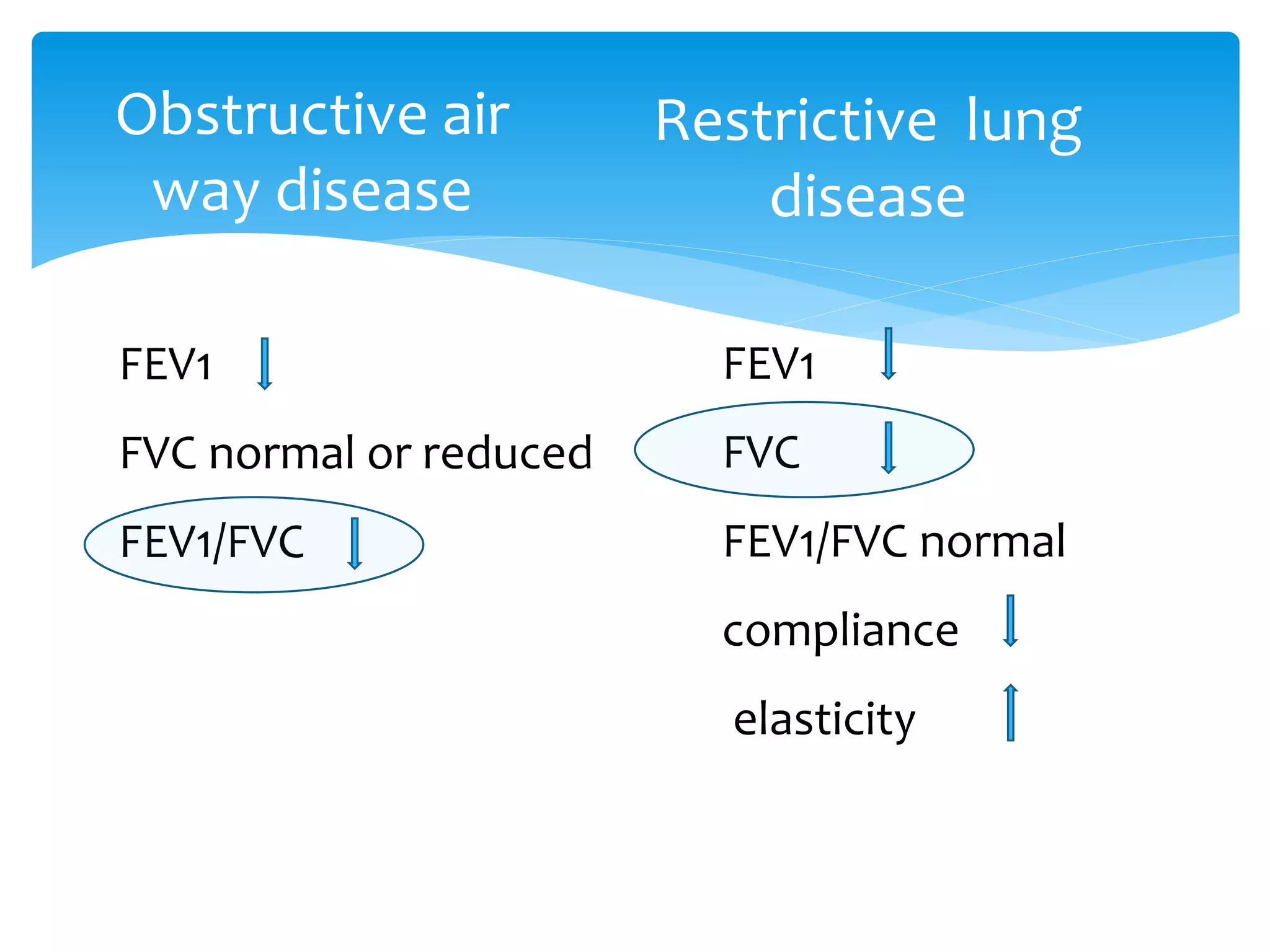
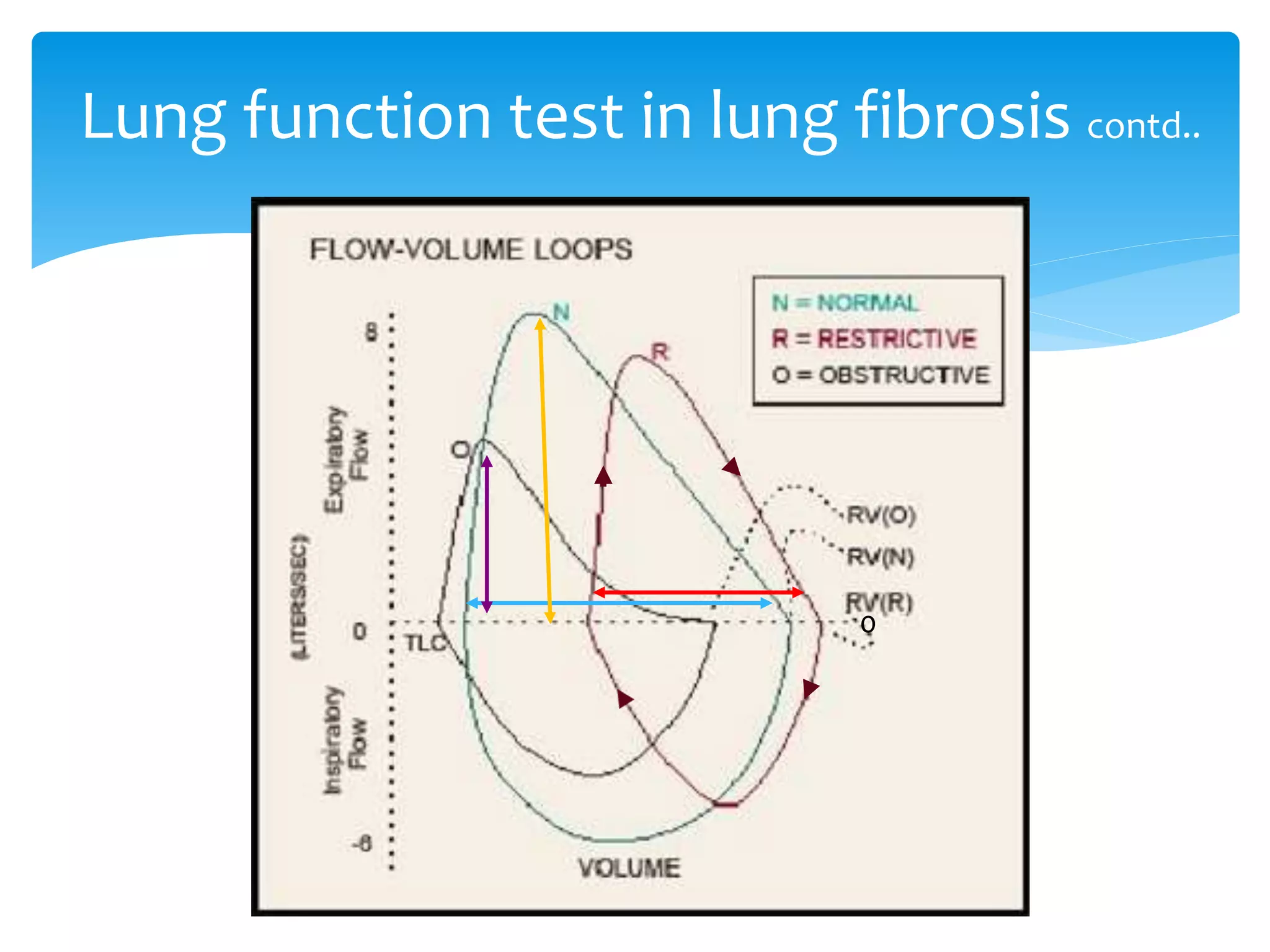






The document discusses restrictive lung disease, outlining its main types, causes, and characteristics, including intrinsic and extrinsic factors affecting lung tissue. It details the diagnosis through lung function tests and compares obstructive airway disease with restrictive lung disease, emphasizing the effects and complications of pulmonary fibrosis. Treatment options are mentioned, highlighting that while pulmonary fibrosis cannot be reversed, certain therapies can alleviate symptoms and slow disease progression.



































































