The document provides information on examining the respiratory system, including:
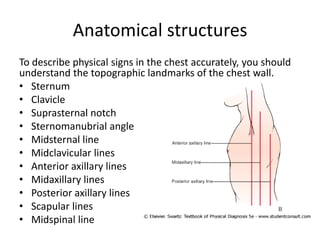
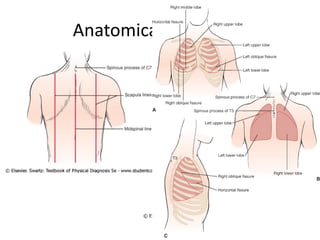
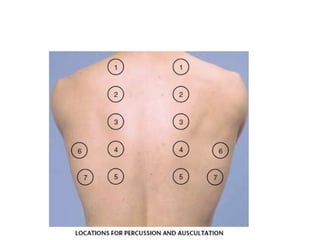
- Key anatomical structures of the chest and how to locate findings
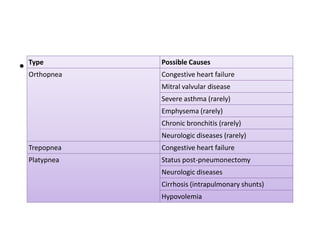
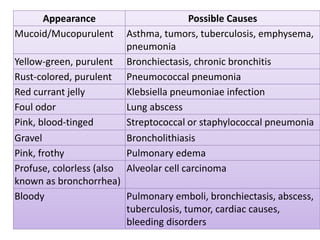
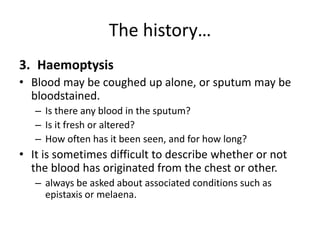
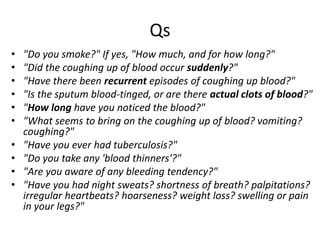
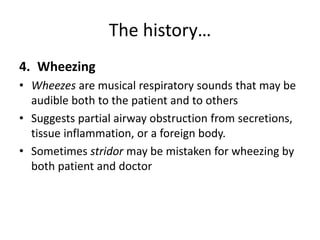
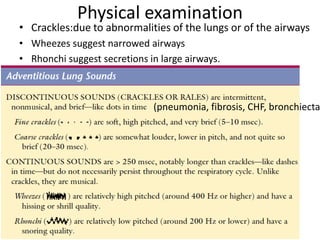
- Main symptoms to ask about including cough, dyspnea, hemoptysis, and wheezing
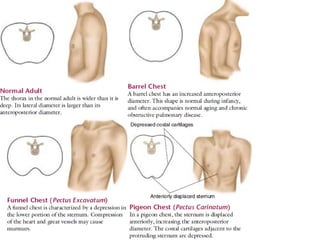
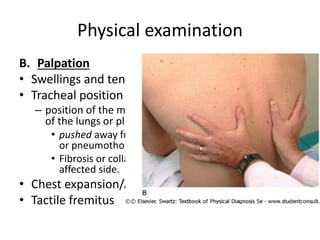
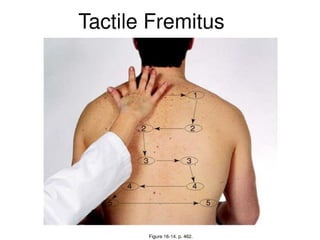
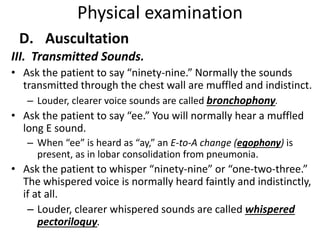
- How to perform a physical exam of the chest including inspection, palpation, percussion, and auscultation
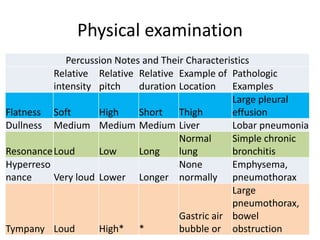
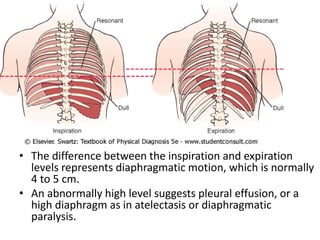
- What different lung sounds and abnormalities indicate















![[Int. med] dyspnoea](https://cdn.slidesharecdn.com/ss_thumbnails/int-150502144320-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)






















































