Downloaded 175 times
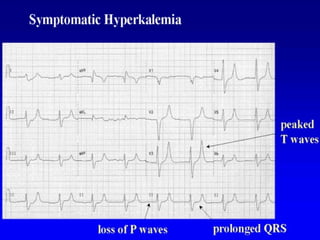
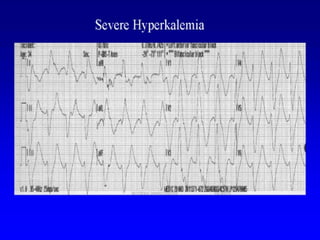
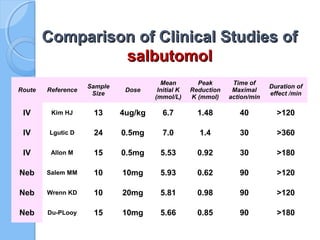
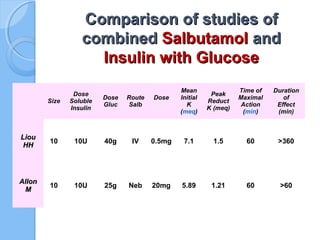
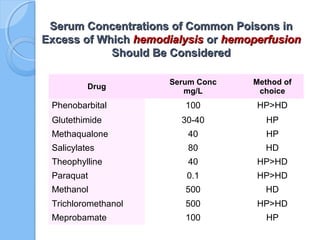


Hyperkalemia is a life-threatening complication in patients with renal failure. Initial management includes calcium gluconate, insulin with glucose, salbutamol, sodium bicarbonate, and sodium polystyrene sulphonate. Hemodialysis is the definitive treatment for severe hyperkalemia. Disequilibrium syndrome is a serious complication of hemodialysis that can cause neurological symptoms. Drug overdoses are commonly treated with hemodialysis or hemoperfusion for water soluble drugs, though dialysis is less effective for lipid soluble or protein-bound substances. Dialysis plays an important role in managing toxic levels of various substances.























































































