The document discusses renal circulation, regulation of renal blood flow, nephron anatomy and physiology, and effects of various drugs on renal function. The key points are:
1) The kidneys receive 20-25% of cardiac output despite only weighing 0.4% of body weight. Renal blood flow is regulated by neural, hormonal and local factors to maintain glomerular filtration.
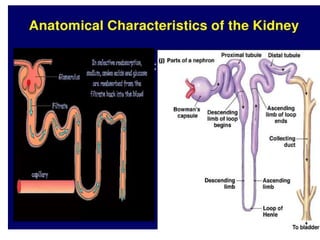
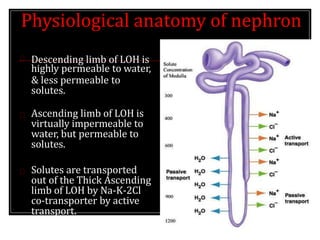
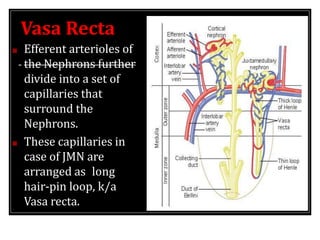
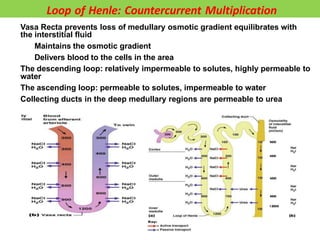
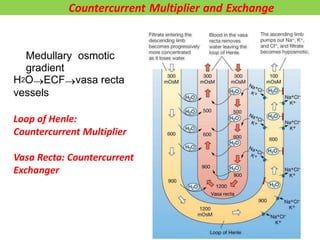
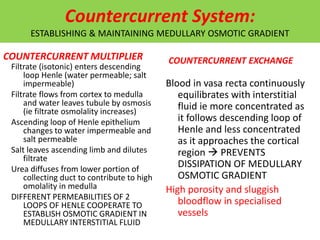
2) Nephrons contain a loop of Henle that acts as a countercurrent multiplier to concentrate urine by establishing an osmotic gradient in the renal medulla, aided by countercurrent exchange in vasa recta capillaries.
3) Drugs like NSAIDs, ACE inhibitors, intravenous agents






































































































![Regulation of urine concentration and volume ].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/regulationofurineconcentrationandvolume-230418093129-e12f4cdf-thumbnail.jpg?width=640&height=640&fit=bounds)


































